

Respirtory (Y2)
Question 1:
Answer: D) Hypocretin (Orexin)
Explanation: Narcolepsy is a neurological disorder characterized by excessive daytime sleepiness, and in some cases, cataplexy (sudden muscle weakness). Hypocretins (orexins) are neuropeptides produced in the hypothalamus. They regulate wakefulness and prevent inappropriate transitions into REM sleep.
A) is incorrect as dopamine is involved in reward and motivation; not directly linked to narcolepsy.
B) is incorrect as serotonin regulates mood and sleep, but its deficiency does not cause narcolepsy.
C) is incorrect as GABA is an inhibitory neurotransmitter; its dysfunction is associated with sleep disorders but not specifically narcolepsy.
E) is also incorrect as acetylcholine plays a role in REM sleep but is not the primary factor in narcolepsy.
Question 2:
Answer: B) Decreased iron levels in the central nervous system
Explanation: Restless Legs Syndrome (RLS) is a neurological disorder characterized by an uncontrollable urge to move the legs, often accompanied by unpleasant sensations. Symptoms are worse at night and during rest. Low iron levels in the brain, particularly in the substantia nigra, affect dopamine synthesis. Iron is a cofactor for tyrosine hydroxylase, the enzyme needed to produce dopamine. Reduced dopamine activity is implicated in RLS, although increased dopamine receptor sensitivity may also contribute. Reduced GABAergic activity may be secondary to iron deficiency, as iron is essential for normal GABA synthesis and function.
A) is incorrect as RLS is linked to reduced dopamine activity, not increased levels.
C) is incorrect as GABAergic function is often decreased in RLS.
D) is incorrect as Low ferritin levels are associated with RLS. Elevated ferritin suggests adequate iron stores and no RLS
E) is incorrect as low serotonin is more closely related to mood disorders; dopamine and iron play central roles in RLS.
Question 3:
Answer: E) Eosinophilic inflammation
Explanation: FeNO is a non-invasive biomarker used to measure airway inflammation, specifically eosinophilic inflammation, in asthma patients. Nitric oxide (NO) is produced by airway epithelial cells in response to inflammation. Elevated FeNO levels indicate increased activity of eosinophils in response to IL-4, IL-5 and IL-13. It helps diagnose asthma and assess corticosteroid responsiveness, usually patients with asthma have high levels of eosinophils before onset of symptoms (since they are variable) if corticosteroids are given prior to symptoms (when FeNO) levels are elevated, the asthma would be more responsive to the medications.
A) is incorrect as FeNO reflects inflammation, not structural changes. Airway remodelling is assessed via imaging or lung function tests.
B) is incorrect as reduced lung function is measured using spirometry (FEV1), not FeNO.
C) is incorrect as FeNO is not a marker for neutrophilic inflammation, which is more common in severe or non-allergic asthma.
D) is incorrect as airway hyperresponsiveness is assessed using challenge tests (e.g., methacholine), not FeNO.
Question 4:
Answer: B) OSA results from airway obstruction, whereas CSA is due to impaired brain signals
Explanation: Obstructive Sleep Apnoea (OSA) is caused by repeated airway obstruction due to soft tissue collapse in the pharynx. The respiratory drive remains intact, but airflow is blocked. Central Sleep Apnoea (CSA) is caused by a loss of respiratory drive from the brainstem, leading to pauses in breathing without airway obstruction.
A) is incorrect as loss of respiratory drive is a characteristic of CSA, not OSA.
C) is incorrect as only OSA involves airway obstruction; CSA does not.
D) is incorrect REM vs. non-REM both conditions can occur in OSA and CSA.
E) is incorrect as snoring is common in OSA, not typically in CSA.
Question 5:
Answer: A) By promoting airway inflammation and oxidative stress
Explanation: PM2.5 refers to fine particulate matter with a diameter of 2.5 micrometres or smaller. Due to their small size, these particles can penetrate deep into the lower respiratory tract and even enter the bloodstream. PM10 are particles that are 10 micrometres or smaller. While larger than PM2.5, they can still enter the upper respiratory system and irritate the airways. There particles contribute to asthma by promoting inflammation and oxidative stress. When inhaled, they penetrate deep into the lungs, triggering an immune response that releases inflammatory cytokines and free radicals, leading to airway damage and worsening asthma.
B) is incorrect as PM2.5 doesn’t directly constrict airway smooth muscles. Inflammation and immune responses are what cause the constriction indirectly.
C) is incorrect as PM2.5 does not increase oxygen absorption; it impairs gas exchange due to lung damage.
D) is incorrect as PM2.5 doesn’t cause immediate bronchospasm. It exacerbates asthma through chronic inflammation and immune activation.
E) is incorrect as PM2.5 can increase mucus production as part of the inflammatory response, not reduce it.
Question 6:
Answer: C) Dexamethasone
Explanation: Dexamethasone is a glucocorticoid which is administered to pregnant women at risk of preterm delivery to stimulate surfactant production in the foetus, reducing the risk of respiratory distress syndrome (RDS).
A) is incorrect because insulin surfactant production. This is why infants of diabetic mothers are at higher risk for RDS.
B) is incorrect because hypoxia inhibits surfactant production and can cause surfactant inactivation, oxygenation however does increase surfactant synthesis.
D) is incorrect as acidosis also inhibits surfactant production.
E) is incorrect as testosterone can delay surfactant maturation, making male preterm infants more prone to RDS.
Question 7:
Answer: D) Transient Tachypnoea of the Newborn (TTN)
Explanation: TTN is a self-limiting respiratory condition due to delayed reabsorption of foetal lung fluid. It’s common in term infants delivered by C-section without labour, as they miss the hormonal and mechanical triggers (thoracic squeeze) that clear lung fluid during vaginal delivery.
A) is incorrect as respiratory distress syndrome (RDS) seen in preterm infants due to surfactant deficiency. X-rays show ground-glass opacities.
B) is incorrect as congenital diaphragmatic hernia (CDH) presents with severe respiratory distress, scaphoid abdomen, and X-rays show bowel loops in the thorax.
C) is incorrect because meconium aspiration syndrome (MAS) occurs in term/post-term infants with meconium-stained amniotic fluid. X-rays show patchy infiltrates and areas of overinflation.
E) is incorrect as Pulmonary Hypoplasia is associated with CDH (congenital diaphragmatic hernia) or prolonged oligohydramnios. X-rays show small, bell shaped, underdeveloped lungs.
Question 8:
Answer: A) Surfactant deficiency
Explanation: Neonatal respiratory distress syndrome (RDS) is primarily due to surfactant deficiency. Surfactant is crucial for reducing alveolar surface tension, allowing the lungs to expand and preventing alveolar collapse (atelectasis). Surfactants are produced by Type II pneumocytes in the lungs, they contain phospholipids and surfactant proteins (SP) such as SP-A and SP-D which are involved in immune defence, helping clear pathogens and regulate surfactant balance, SP-B and SP-C which are essential for adsorption and spreading of surfactant on alveolar surfaces.
B) is incorrect as Transient Tachypnoea of the Newborn (TTN) is caused by delayed clearance of foetal lung fluid. It presents with mild respiratory distress and normal surfactant levels. X-rays show fluid in the fissures, not ground-glass opacities. TTN would be likely in a term baby born by C-section without labour, presenting with tachypnoea but resolving in 24-48 hours.
C) is incorrect as Meconium Aspiration Syndrome (MAS) occurs when the infant inhales meconium-stained amniotic fluid (amniotic fluid with faeces), often in term or post-term babies. X-rays show patchy infiltrates, not uniform ground-glass.
D) is incorrect as Congenital Diaphragmatic Hernia (CDH) involves abdominal organs herniating into the thoracic cavity, impairing lung development (pulmonary hypoplasia). X-rays show bowel loops in the chest.
E) is incorrect as Pulmonary Hypoplasia is the underdevelopment of lung tissue and is often secondary to CDH or oligohydramnios. It leads to severe respiratory failure, but X-rays show small lung volumes and bell-shaped lungs rather than classic RDS findings.
Question 9:
Answer: E)6
Explanation:
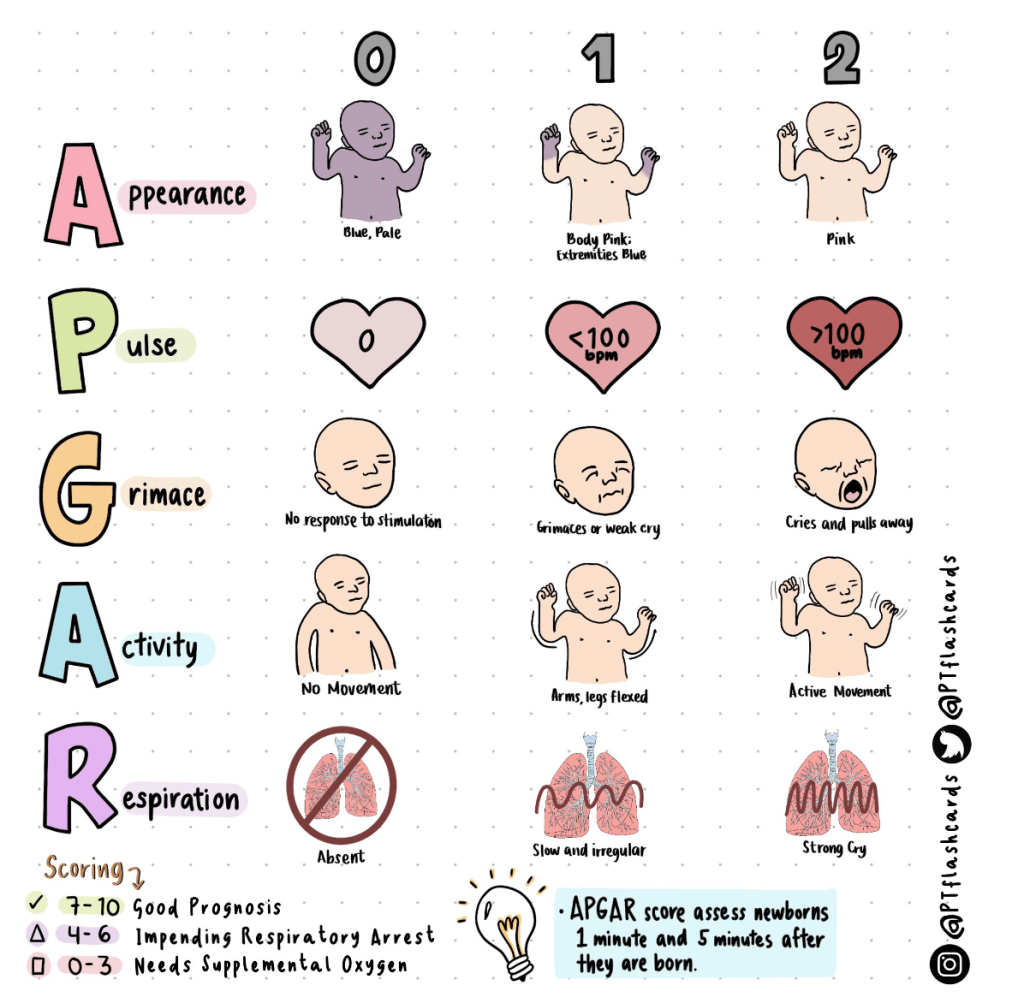
Scoring Calculation:
Heart Rate: 2 points (HR > 100 bpm)
Respiration: 1 point (weak, irregular breathing)
Muscle Tone: 1 point (some flexion)
Reflex Irritability: 1 point (weak cry)
Colour: 1 point (blue extremities)
Total APGAR Score:
2 + 1 + 1 + 1 + 1 = 6 points
Question 10:
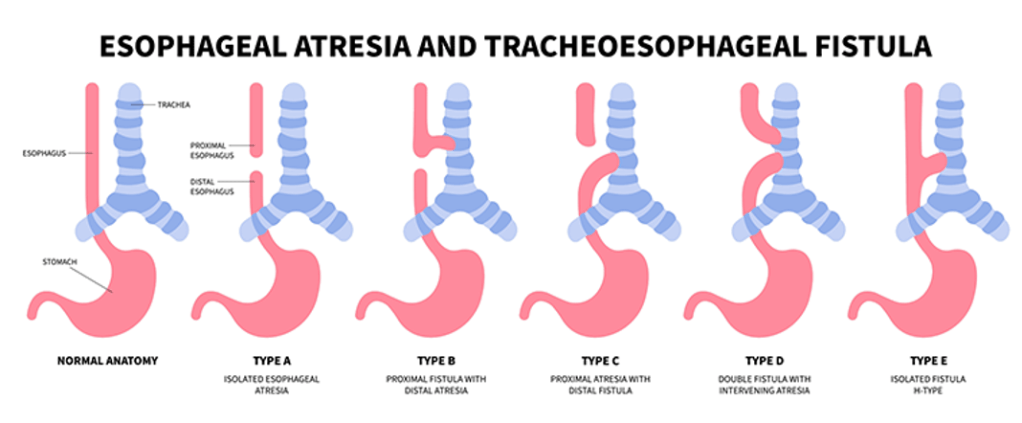
Answer: B) Coiling of a nasogastric (NG) tube on X-ray
Explanation: In tracheoesophageal fistula (TEF) with oesophageal atresia, an NG tube cannot pass into the stomach. Instead, it coils in the upper oesophageal pouch, visible on X-ray.
Clinical Features include:
- Excessive drooling and salivation.
- Choking and cyanosis during feeding.
- Inability to pass NG tube into the stomach.
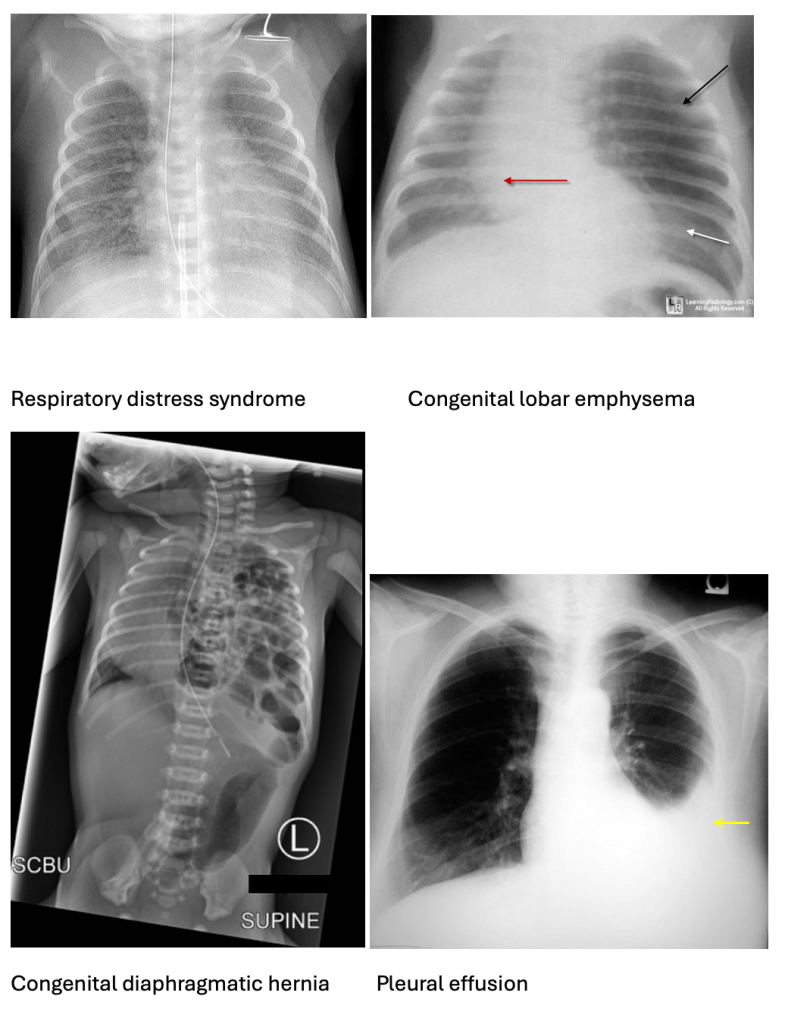
A) is incorrect as ground-glass appearance: Indicates RDS- respiratory distress syndrome.
C) is incorrect as hyperinflated left upper lobe is seen in CLE – congenital lobar emphysema.
D) is incorrect as bowel loops in the thorax suggests CDH- congenital diaphragmatic hernia.
E) is incorrect as pleural effusion is fluid in the pleural cavity, not related to TEF.
Question 11:
Answer: D) They prevent the clot from growing and allow the body to break it down naturally.
Explanation: Anticoagulants (like heparin and warfarin) work by interfering with the clotting cascade. This prevents the formation of new clots and stops existing clots from getting bigger in smaller emboli, however they do NOT lyse them like tPA (Tissue plasminogen activators which are used in thrombolytic treatment for massive pulmonary embolisms). The body’s natural fibrinolytic system (involving plasmin) gradually breaks down the clot over time.
A) is incorrect as dissolving the blood clot immediately is referring to thrombolytic therapy, such as tPA (tissue plasminogen activator), which actively dissolves blood clots. Thrombolytics are used in life-threatening situations like massive pulmonary embolism (PE) because they work quickly but carry a high risk of bleeding.
B) is incorrect because activation of plasmin to break down the clot directly is the function of thrombolytics like tPA. They convert plasminogen into plasmin, which breaks down fibrin in the clot, whereas anticoagulants do not activate plasmin; they prevent clotting by inhibiting factors in the clotting cascade.
C) is incorrect because the physical removal of a clot from the pulmonary artery describes an embolectomy, a surgical or catheter-based procedure. It’s reserved for severe cases where other treatments fail or when the patient is too unstable for thrombolytics.
E) is incorrect because filtration of blood clots from the inferior vena cava (IVC) is what an IVC filter does, it is a device implanted in the inferior vena cava to trap clots traveling from the lower body to the lungs. However, it doesn’t treat existing clots; it prevents future pulmonary embolisms.
Question 12:
Answer: C) D-dimer test
Explanation: D-dimer is a fragment of fibrin produced when a clot is broken down by plasmin. Elevated D-dimer levels indicate that the body is actively breaking down clots. A normal D-dimer (whereby levels are below 500) can rule out PE, but an elevated D-dimer (where levels are above 500) requires further testing (e.g., CT pulmonary angiogram) because it can be elevated in many conditions like myocardial infarction or sepsis.
A) is incorrect because a complete blood count (CBC) measures the levels of red blood cells, white blood cells, and platelets. It does not assess clot breakdown or fibrinolysis. CBS is useful for detecting anaemia or infection but not for diagnosing PE.
B) is incorrect because prothrombin time (PT) measures how long it takes blood to clot. It’s used to monitor warfarin therapy. However, it doesn’t measure fibrin breakdown or diagnose PE.
D) is incorrect as arterial blood gas (ABG) measures oxygen and carbon dioxide levels in the blood. It helps assess respiratory function such as if there is acidosis or alkalosis and whether it is respiratory or metabolic but does not detect clots or fibrin breakdown.
E) is incorrect because troponin is a marker of heart muscle damage, primarily used to diagnose myocardial infarction (heart attack), but it is not used to detect fibrin breakdown.
Question 13:
Answer: A) Sudden onset of dyspnoea
Explanation: Dyspnoea is the most common symptom of PE. It can occur suddenly and without warning, making it a key diagnostic clue. Sudden dyspnoea can occur because the pulmonary artery is blocked by a clot, reducing blood flow to the lungs, the blockage increases pulmonary vascular resistance, straining the right ventricle. This leads to a reduction in blood flow causing to a mismatch between ventilation and perfusion (V/Q mismatch due to dead space), and therefore hypoxemia (low blood oxygen). The body compensates by increasing breathing rate (tachypnoea) to improve oxygen intake.
B) is not the best answer because it is a rare symptom of PE, it occurs when the clot causes pulmonary infarction (death of lung tissue). The obstruction of a pulmonary artery leads to reduced blood supply, causing tissue necrosis and rupture of small blood vessels. This bleeding then enters the airways, resulting in haemoptysis. Haemoptysis is usually a more common finding in tuberculosis (TB), lung cancer, bronchiectasis due to chronic infection causing a bleed, acute bronchitis where severe coughing can irritate airways, causing minor bleeding. But sudden dyspnoea is the most common clinical presentation of PE.
C) is not the best answer either because it’s not the most common presentation.
In PE, cyanosis occurs when the clot significantly reduces oxygenation of the blood. This is typically seen in large or multiple emboli that severely impair lung function. It indicates severe hypoxia and is usually a late sign. If present, it suggests a large PE or advanced respiratory failure and immediate intervention is required.
D) is not the best answer because a productive cough involves mucus (sputum) being expelled from the lungs. It is common in infections like pneumonia or bronchitis, not PE. PE typically causes a dry cough due to irritation of the pleura (lining around the lungs). A productive cough may indicate:
E) is incorrect because bradycardia refers to a slow heart rate (usually <60 bpm). In PE, the body compensates for reduced oxygen by increasing the heart rate (tachycardia). This improves blood flow and oxygen delivery. Bradycardia is rare and may indicate severe right ventricular strain as if the heart is failing, it may slow down.
Question 14:
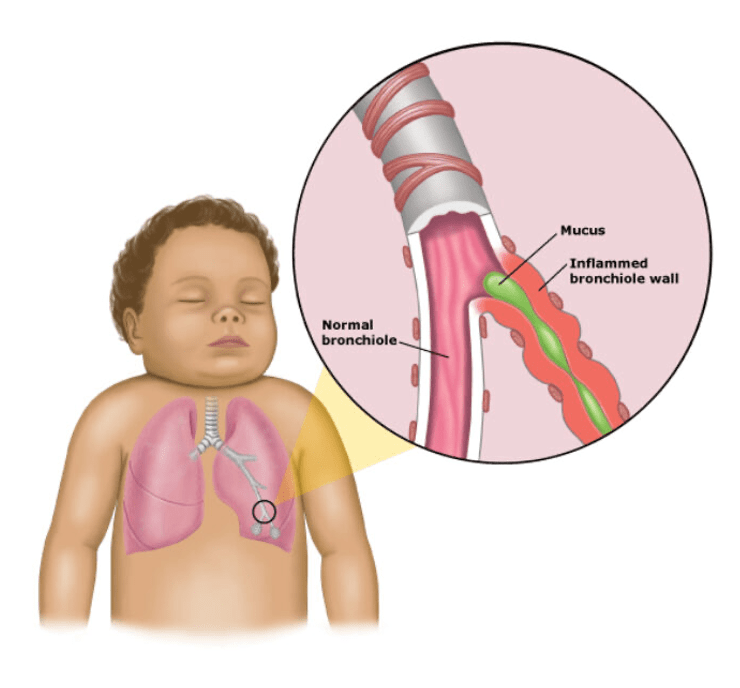
Answer: E) Respiratory Syncytial Virus (RSV)
Explanation: RSV is the leading cause of bronchiolitis, especially in children younger than 1 year. It causes inflammation in the small airways (bronchioles), leading to symptoms such as wheezing, coughing, and respiratory distress. RSV is highly contagious and commonly peaks in winter months, making it the most common viral cause of bronchiolitis in infants. It’s known for causing the swelling and mucus buildup in the small airways, which leads to wheezing and difficulty breathing.
A) is incorrect as Influenza virus usually leads to respiratory illnesses, including pneumonia, but it is not the most common cause of bronchiolitis in infants. Influenza tends to cause more general viral UPPER respiratory symptoms or flu-like illness, and it can affect people of all ages. However, it is not specifically known for causing bronchiolitis, which primarily affects the small airways.
B) is incorrect as Adenovirus can cause a range of respiratory infections, including pneumonia and bronchitis, but it is not the primary cause of bronchiolitis in infants.
C) is not the best answer because Parainfluenza virus can cause a variety of respiratory infections which does include bronchiolitis, but they are typically associated with conditions like croup (which causes a barking cough) and upper respiratory infections. While it can contribute to bronchiolitis, it is not as common as RSV, so it is not the best answer.
D) is incorrect as Rhinovirus is the main cause of the common cold, and while it can cause mild respiratory infections in infants, it is not generally known for causing bronchiolitis. It primarily causes upper respiratory tract symptoms like nasal congestion and a runny nose.
Question 15:
Answer: B) Syncytial giant cells
Explanation: Syncytial giant cells are a hallmark finding in RSV infections. These are multinucleated cells that form when individual infected epithelial cells in the airways fuse together due to the virus. This fusion of cells is a result of the viral infection itself. These cells are key diagnostic features in the histological examination of bronchiolitis caused by RSV.
A) is incorrect because eosinophilic granulomas are typically associated with allergic reactions or hypersensitivity pneumonitis. In these conditions, eosinophils accumulate in response to allergens or irritants. RSV-induced bronchiolitis does not typically feature eosinophilic granulomas.
C) is incorrect because necrotizing granulomas are a type of chronic inflammation often seen in mycobacterial infections (e.g., tuberculosis) or fungal infections (e.g., histoplasmosis or aspergillosis). These granulomas are associated with necrosis as part of a chronic immune response. RSV-induced bronchiolitis typically does not cause granulomas, let alone necrotizing ones.
D) is not the best answer as although macrophages are involved in the immune response to RSV infection, they do not constitute a major histological feature of RSV-induced bronchiolitis. Macrophages are important in inflammation and debris clearance, but the defining feature of RSV infection is the formation of syncytial giant cells, not macrophage accumulation.
E) is incorrect because pus-filled abscesses are typically associated with bacterial infections rather than viral infections like RSV. In RSV-induced bronchiolitis, the inflammation is viral in nature, and there is no formation of abscesses. Pus formation would be more characteristic of a bacterial pneumonia or lung abscess.
Question 16:
Answer: B) Fibrosis of the parenchyma
Explanation: Asbestosis is characterized by fibrosis (scarring) of the lung parenchyma due to prolonged asbestos exposure. This can lead to restrictive lung disease, decreased lung function, and dyspnoea (shortness of breath). It can also increase the risk of developing lung cancer.
A) is incorrect because acute exacerbation of asthma is typically triggered by allergens and inflammatory responses in the airways. Asbestosis, a chronic lung condition caused by asbestos exposure, is not characterized by asthma exacerbations.
C) is incorrect because Pneumonia is not a major concern in asbestosis. While pneumonia is a possible secondary infection in any person with lung disease, asbestosis is characterized by fibrosis (scarring) of the lungs due to asbestos exposure, not an acute infection.
D) is incorrect because Pulmonary embolism is not a typical concern in asbestosis, which primarily affects the lung parenchyma (tissue) and causes fibrosis. It is more commonly seen in conditions like deep vein thrombosis (DVT) or cardiac disease.
E) is incorrect because pleural plaques are a benign finding associated with asbestos exposure, but they are not a major cause of concern in asbestosis. They are usually asymptomatic, although they can serve as an indicator of past asbestos exposure.
Question 17:
Answer: C) Z-score < -1.64
Explanations: A Z-score of less than -1.64 is concerning, it indicates a significant decrease in lung function, which is alarming because it suggests that the patient’s airway function is impaired and that there is severe obstruction. This would likely reflect inadequate asthma control, severe asthma, or worsening of asthma, which may require intensified management or closer monitoring.
A) is incorrect as a Z-score > 1.64 indicates better-than-expected lung function compared to a healthy population. This would not be concerning in asthma, as it suggests normal or improved lung function.
B) is incorrect as a Z-score between 0 and 1.64 is generally normal, indicating that the patient’s lung function is within expected limits for their age, height, and sex. This is not typically concerning in asthma unless symptoms worsen.
D) is incorrect as a Z-score between -1.64 and 0 suggests borderline abnormality, where the Z-score is slightly below normal, but not drastically abnormal. It may indicate early signs of airway obstruction or declining function, but not necessarily severe asthma.
E) is incorrect as a Z-score > 2.5 would indicate exceptionally high lung function, well above the expected norm. This would be uncommon and unlikely to be seen in asthma, where airway obstruction would usually lower the Z-score.
Question 18:
Answer: D) High fever, elevated inflammatory markers, and multi-organ involvement
Explanation: The hallmark of PIMS-TS is a high fever, elevated inflammatory markers, and multi-system involvement, which may include cardiac, renal, gastrointestinal, and dermatologic issues.
A) is incorrect because a mild fever with normal inflammatory markers is not typical of PIMS-TS, as the syndrome usually involves high fever and elevated inflammatory markers (like CRP and ESR).
B) is incorrect as a localized rash limited to the face is not characteristic of PIMS-TS, where a widespread rash can occur, often in the form of a maculopapular or erythematous rash.
C) is incorrect as although mild gastrointestinal upset (e.g., abdominal pain, diarrhoea) can occur, they alone are not sufficient to suggest PIMS-TS. PIMS-TS typically presents with more severe systemic inflammation.
E) is incorrect as elevated WBC count with normal platelets is atypical, a typical finding in PIMS-TS is elevated WBC and low platelet count, so normal platelets would be less consistent with this syndrome.
Question 19:
Answer: C) Epiglottitis
Explanation: Epiglottitis is a severe, life-threatening condition usually caused by Haemophilus influenzae type B (Hib). It leads to inflammation of the epiglottis, causing a narrowing of the airway. The biphasic stridor (both inspiratory and expiratory) occurs because the obstruction is severe and fixed. Other symptoms include drooling, a high fever, sitting forward, leaning on hands to breathe easier.
A) is incorrect because croup causes inspiratory stridor, a barking cough and hoarseness. The stridor is not biphasic in croup, it is inspiratory. Croup is a viral infection (usually due to parainfluenza virus).
B) is incorrect as Asthma presents with wheezing (especially during expiration), shortness of breath, and chest tightness. There is no stridor because asthma affects the lower airways, not the upper airway.
D) is incorrect because Bronchiolitis causes wheezing, crackles and coughing but not stridor. Bronchiolitis is a viral infection (commonly caused by RSV) affecting the small airways – bronchioles.
E) is incorrect as Pneumonia causes symptoms like fever, productive cough and crackles on auscultation, it does NOT cause stridor. Pneumonia is an infection of the alveoli.
Question 20:
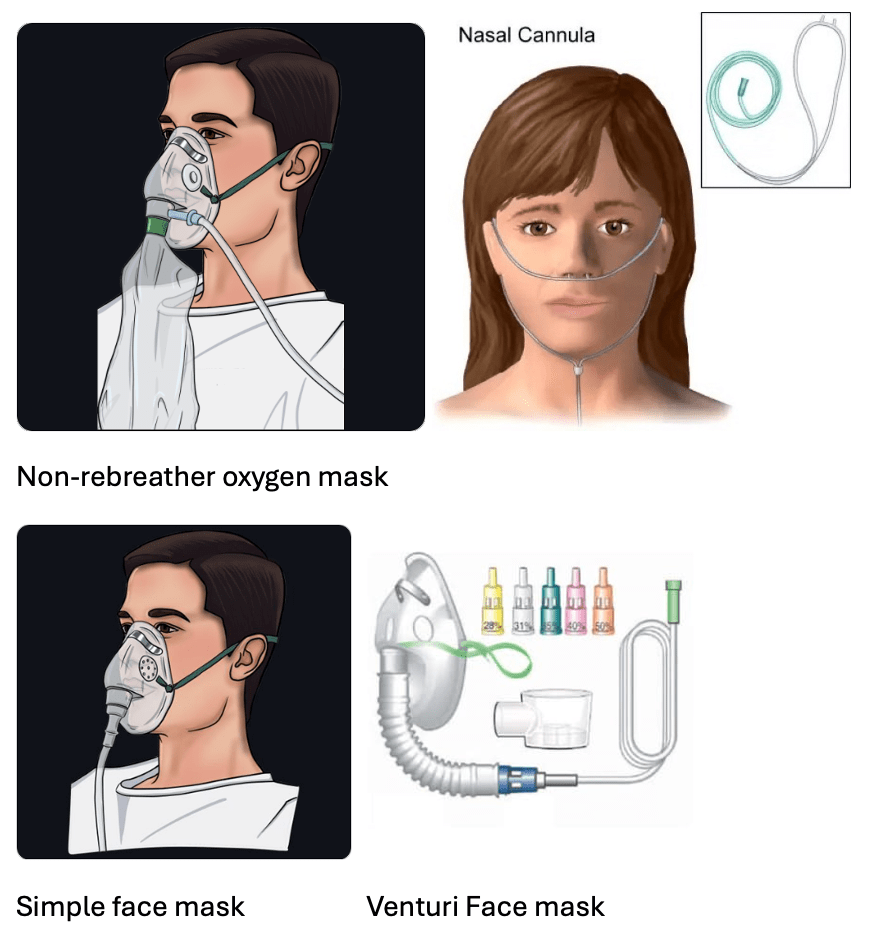
Answer: D) non-rebreather mask
Explanation: A non-rebreather mask provides the highest concentration of oxygen (up to 90-100%). It has a reservoir bag that fills with oxygen and a one-way valve to prevent exhaled air from re-entering the bag. The non-rebreather mask is used in acute hypoxia or medical emergencies.
A) is incorrect as a nasal cannula is a device delivers low-flow oxygen at concentrations of about 24-40%, depending on the flow rate (1-6 L/min). It’s suitable for patients with mild hypoxia who need long-term oxygen therapy.
B) is incorrect as a simple face mask delivers 40-60% oxygen at flow rates of 5-10 L/min. It’s used when a higher concentration than a nasal cannula is needed but doesn’t provide the highest oxygen levels.
C) is incorrect as a Venturi mask delivers precise oxygen concentrations (from 24% to 60%) by mixing oxygen with room air. It’s often used in patients with COPD to prevent hypercapnia (high CO₂ levels).
E) is incorrect as CPAP (Continuous Positive Airway Pressure) maintains continuous pressure in the airways, preventing collapse and improving oxygenation in conditions like sleep apnoea or pulmonary oedema. However, it doesn’t deliver the highest oxygen concentration directly.
Question 21:
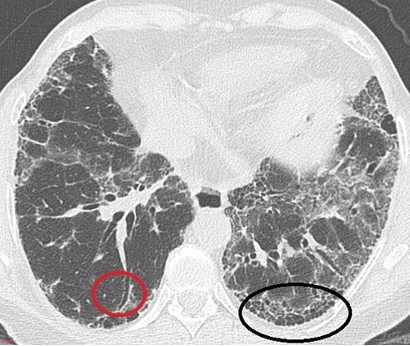
Answer: A) Honeycombing pattern in the lungs
Explanation: IPF is characterised by a honeycombing pattern on CT and lung biopsy. This pattern indicates the presence of fibrotic cystic spaces within the lung, a key diagnostic feature of Usual Interstitial Pneumonia (UIP), which is the histopathological pattern seen in IPF.
B) is incorrect as non-necrotizing granulomas are characteristic of sarcoidosis, not IPF. They are aggregates of immune cells without tissue necrosis, often found in the lungs and lymph nodes.
C) is incorrect as caseating granulomas are associated with tuberculosis or certain fungal infections like histoplasmosis. Caseation refers to necrosis with a cheese-like appearance.
E) is incorrect as extensive mucus production in the bronchioles describes conditions like chronic bronchitis or bronchiectasis, not IPF.
Question 22:
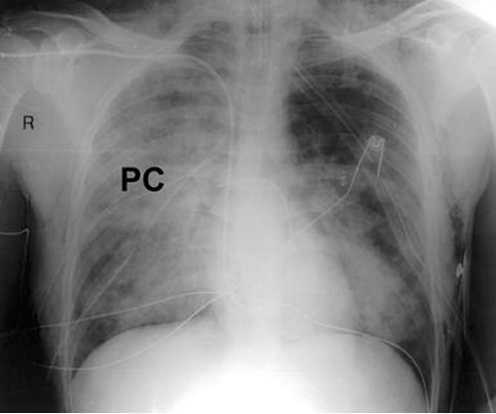
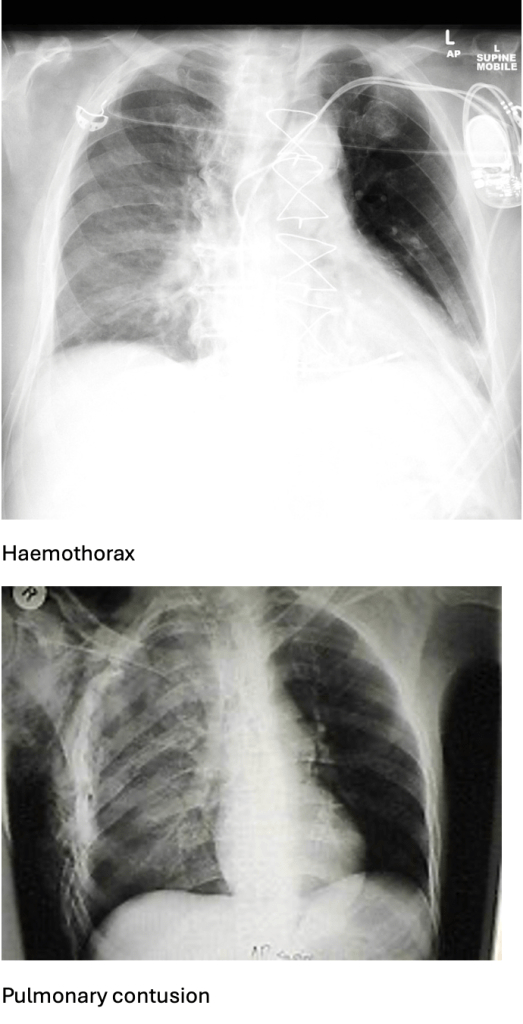
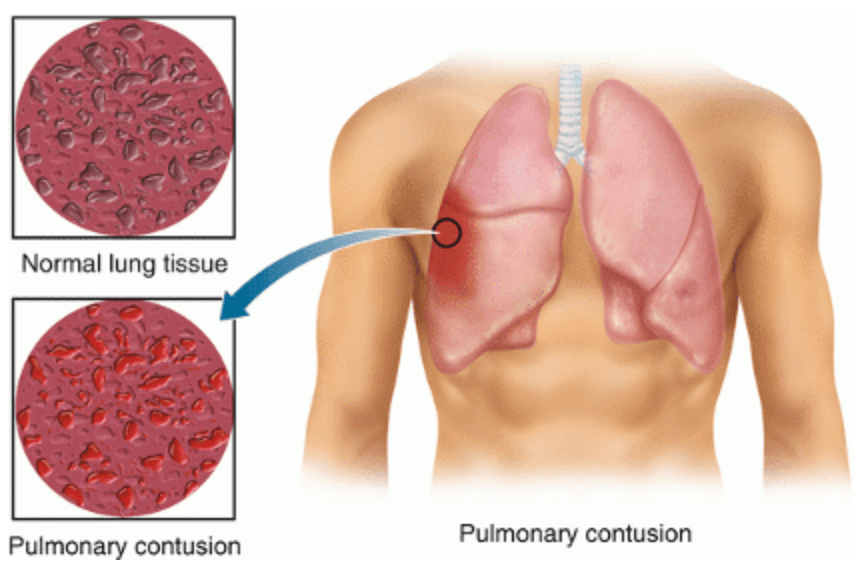
Answer: B) Pulmonary contusion
Explanation: A pulmonary contusion occurs after direct impact to the chest compresses lung tissue. This causes rupture of alveolar capillaries and bleeding into the alveoli. The resulting inflammatory response leads to oedema and accumulation of blood in the lung parenchyma. Clinical features include dyspnoea, haemoptysis, and crackles.
A) is incorrect because tension pneumothorax presents with severe respiratory distress, tracheal deviation away from the affected side, and reduced breath sounds on one side. There’s no mention of these key signs.
C) is incorrect as a simple pneumothorax would show a collapsed lung on X-ray, with absent breath sounds on the affected side but no infiltrates. Haemoptysis is uncommon.
D) is incorrect as haemothorax usually presents with dullness to percussion and evidence of fluid on X-ray. Infiltrates indicate alveolar injury, not fluid collection.
E) is incorrect because flail chest requires multiple rib fractures, leading to paradoxical chest movement, this is not mentioned in the scenario.
Question 23:
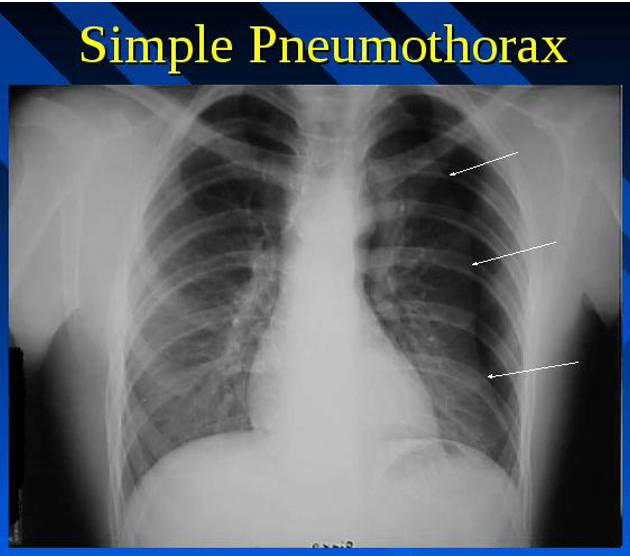
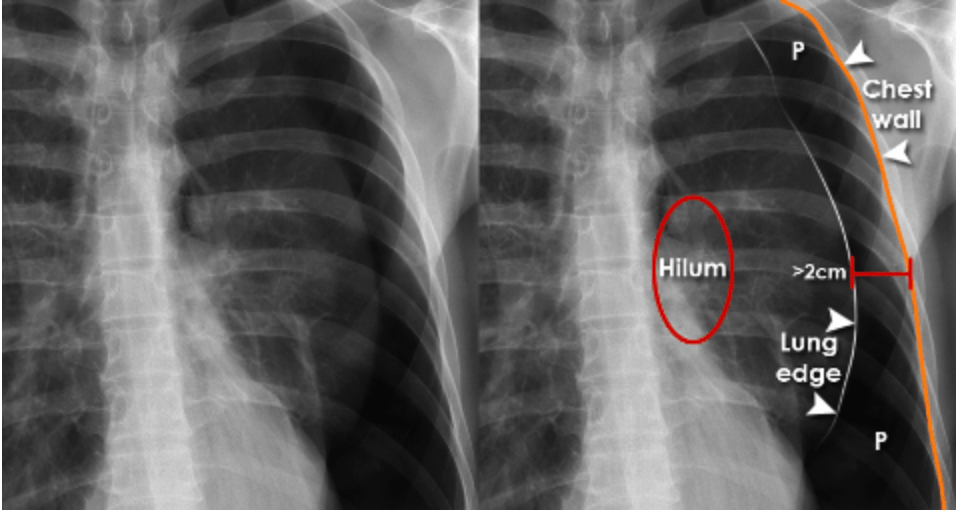
Answer: E) Simple pneumothorax
Explanation: A simple pneumothorax occurs when air enters the pleural space, causing lung collapse without mediastinal shift. Reduced breath sounds on one side and an absence of lung markings on X-ray confirm this. No tracheal deviation means it’s not tension pneumothorax.
A) is incorrect as tension pneumothorax would present with tracheal deviation away from the affected side, severe respiratory distress, and hypotension.
B) is incorrect because a flail chest requires multiple rib fractures causing a floating segment and paradoxical chest wall movement (ribs move in on inspiration and out on expiration.
C) is incorrect as haemothorax is characterised by dullness to percussion and an opacity on X-ray due to blood accumulation.
D) is incorrect as pulmonary contusion causes patchy infiltrates on X-ray and often follows blunt trauma with no pleural space involvement.
Question 24:
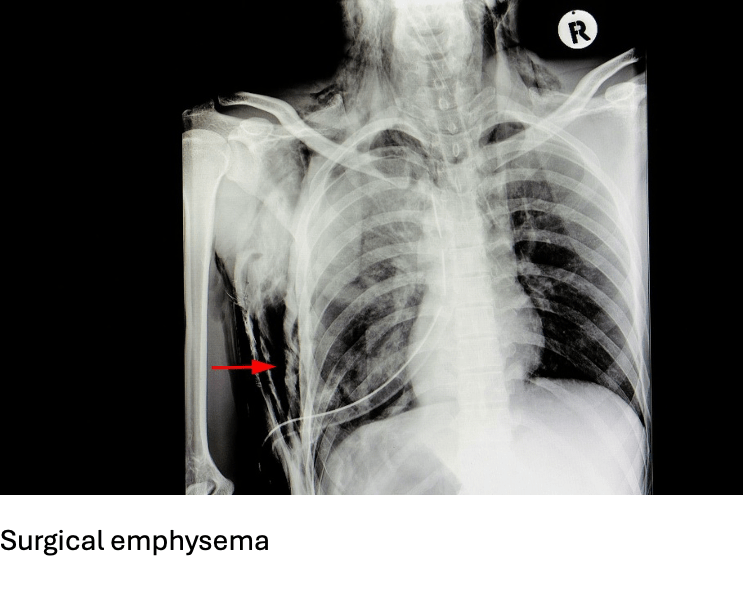
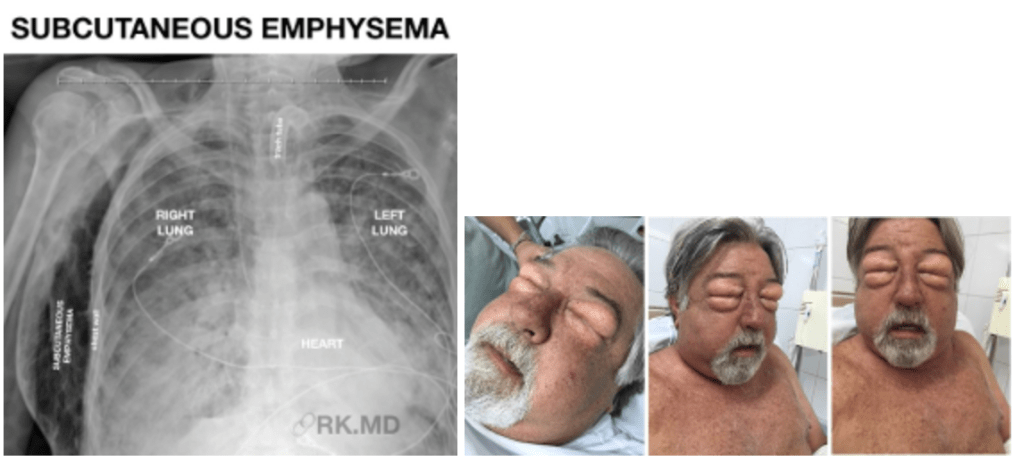
Answer: A) Air leakage into subcutaneous tissue
Explanation: Surgical emphysema (or subcutaneous emphysema) occurs when air leaks into the subcutaneous tissue, usually from chest trauma or pneumothorax. It causes crepitus (crackling sensation) under the skin.
B) is incorrect because air trapped in the pleural space describes a pneumothorax.
C) is incorrect because bleeding into the pleural cavity describes a haemothorax.
D) is incorrect because multiple rib fractures causing paradoxical chest movement is a characteristic of flail chest.
E) is incorrect as lung tissue damage with oedema from blunt trauma describes a pulmonary contusion.
Question 25:
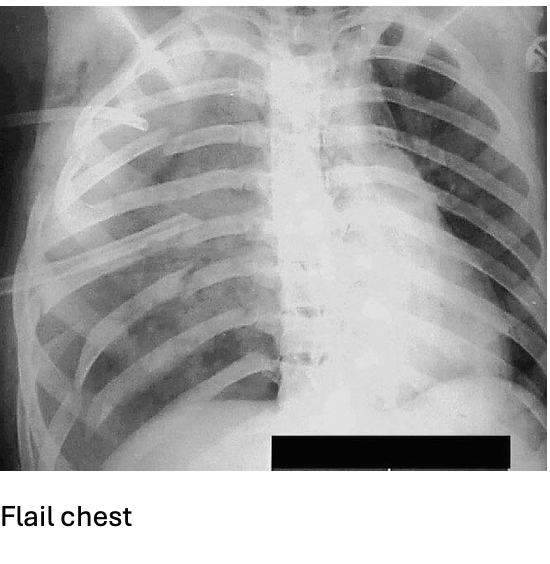
Answer: D) Flail chest
Explanation: Flail chest occurs when multiple rib fractures create a segment that moves paradoxically – inward during inspiration and outward during expiration. This disrupts normal ventilation.
A) is incorrect as tension pneumothorax causes tracheal deviation and severe respiratory distress.
B) is incorrect as haemothorax involves blood in the pleural space without paradoxical motion.
C) is incorrect as pulmonary contusion is due to alveolar injury causing oedema, without rib fracture paradoxical movement.
E) is incorrect as a simple pneumothorax involves air in the pleural space with no abnormal chest wall movement.
Question 26:
Answer: B) It blocks the breakdown of cyclic AMP (cAMP), reducing inflammation.
Explanation: Roflumilast is a PDE4 inhibitor. PDE4 is an enzyme that breaks down cAMP, which plays a key role in controlling inflammation in the body. By blocking PDE4, roflumilast increases the levels of cAMP, which in turn reduces inflammation in the airways of people with COPD by inhibiting the release of proinflammatory cytokines and chemokines. This helps in decreasing exacerbations and controlling long-term symptoms.
A) is incorrect as beta-2 blockers are what inhibits beta-2 adrenergic receptors to cause bronchoconstriction, not PDE4 inhibitors like roflumilast. Roflumilast works on cAMP levels, not directly on beta receptors.
C) is incorrect as LABA is what works by stimulating beta-2 receptors to relax airway muscles, not by increasing cAMP through PDE4 inhibition.
D) is incorrect because Roflumilast reduces inflammation and affects immune cell activation, but it does not directly reduce the number of neutrophils in circulation.
E) is incorrect because Roflumilast does not increase corticosteroid production; instead, it works to modulate inflammatory pathways via cAMP.
Question 27:
Answer: A) ICS reduce inflammation and prevent β-agonist receptor desensitization by restoring receptor numbers.
Explanation: ICS (Inhaled Corticosteroids) help reduce inflammation in the airways. LABAs (Long-Acting Beta-2 Agonists) work by stimulating β-receptors, leading to bronchodilation. However, long-term use of LABAs can lead to β-receptor desensitization, meaning the receptors become less responsive to the drug. ICS help reverse this by increasing the number of β-receptors, making them more sensitive to LABA, thus improving the long-term effectiveness of LABAs. This synergistic effect of ICS and LABA is beneficial for treating COPD.
B) is incorrect because ICS do not act on β-receptors. They work by reducing inflammation and enhancing the responsiveness of β-receptors to LABA.
C) is incorrect because ICS reduce inflammation, not increase cytokines which would increase inflammation. The combination of ICS and LABA works through anti-inflammatory effects (ICS) and bronchodilation (LABA).
D) is incorrect because ICS do not completely prevent the synthesis of inflammatory cells; they reduce their activation, also LABA cause bronchodilation, not vasoconstriction.
E) is incorrect because ICS can reverse the desensitization of β-receptors caused by LABA by increasing their numbers and enhancing their sensitivity through preventing the uncoupling of the receptors from their associated GPCRs.
Question 28:
Answer: C) Oral corticosteroids are typically used for acute exacerbations of COPD.
Explanation: Oral corticosteroids (e.g., prednisone) are generally reserved for acute exacerbations of COPD because they are more systemic in action, providing stronger anti-inflammatory effects when used in high doses. ICS are used for chronic management, as they target inflammation in the airways more locally with fewer systemic effects.
A) is not the best answer as although oral corticosteroids are potent, they also have more systemic side effects, such as weight gain, osteoporosis, and diabetes, so they are not used as first-line treatment for chronic management. ICS are preferred for long-term control.
B) is incorrect because oral corticosteroids are used in acute situations, not for chronic management. If a patient cannot tolerate inhalers, they may be given other options (e.g., nebulizers), not oral steroids.
D) is incorrect as although ICS are helpful for chronic management of COPD, oral corticosteroids are often needed during acute exacerbations to rapidly reduce inflammation.
E) is incorrect because oral corticosteroids are typically used for acute flare-ups, not for mild or stable COPD. ICS or other bronchodilators are preferred for long-term management.
Question 29:
Answer: C) Acute epiglottitis
Explanation:
This 5-year-old boy presents with several key features that suggest acute epiglottitis:
- Harsh, high-pitched inspiratory noise: This is known as stridor, which is typically associated with airway obstruction.
- Worsening on inspiration: The symptoms are worse during inspiration, indicating upper airway obstruction, which is consistent with epiglottitis.
- Sitting forward with neck extended: This position, called the tripod position, is commonly seen in children with upper airway obstruction as they try to improve their breathing.
- Chest indrawing: This suggests severe respiratory distress and indicates the child is struggling to breathe, a hallmark of acute airway obstruction.
- Fever: The fever that started earlier in the day points towards an infectious cause, which is characteristic of acute epiglottitis, caused by Haemophilus influenzae type b (Hib) or other bacterial infections.
Option A – Laryngomalacia is incorrect because Laryngomalacia is a condition where there is softening of the laryngeal cartilage, causing intermittent stridor, typically worse during expiration rather than inspiration. It is a chronic condition and usually presents in infants, not typically in a well-appearing 5-year-old with acute symptoms like fever and respiratory distress.
Option B is incorrect because foreign body aspiration can cause sudden-onset stridor and respiratory distress. However, it typically causes unilateral wheezing or stridor due to obstruction of one side of the airway. The key finding here is the fever, which is more suggestive of an infection (such as in epiglottitis), rather than foreign body aspiration. Foreign body aspiration generally does not present with fever or a systemic illness, which makes it less likely in this case.
Option D is incorrect because chronic inspiratory stridor is a general term for ongoing upper airway noise. However, the presence of acute symptoms like fever, severe respiratory distress, and the tripod position points toward an acute infectious process like acute epiglottitis rather than a chronic condition. Chronic inspiratory stridor often implies a non-acute condition, and the boy’s presentation is much more severe and acute in nature.
Option E is incorrect because viral respiratory infections, such as croup, can cause stridor and fever. However, croup tends to cause mild to moderate symptoms and does not cause severe respiratory distress with signs of airway obstruction like indrawing of the chest, the tripod position, or the high-pitched inspiratory noise described in this case. It generally presents on expiration not inspiration. Also, croup usually affects younger children (typically 6 months to 3 years) and presents with a characteristic barking cough, which is not mentioned in this scenario. Therefore, a viral respiratory infection is less likely in this child.
Question 30:
Answer: B) Pulmonary oedema
Explanation:
This 72-year-old man with a history of chronic heart failure presents with worsening shortness of breath and fatigue. On auscultation, fine crackles at the lung bases are heard, which strongly suggest pulmonary oedema. Pulmonary oedema occurs when fluid accumulates in the alveoli due to left-sided heart failure. In left-sided heart failure, the left ventricle’s inability to pump blood effectively causes increased pressure in the pulmonary veins, leading to fluid leakage into the lungs. This results in fine crackles, particularly at the lung bases, and is associated with symptoms such as shortness of breath, fatigue, and orthopnea.
Option A is incorrect because bronchitis typically presents with a productive cough, wheezing, and discomfort in the chest, not fine crackles. Bronchitis is caused by inflammation of the airways and does not typically cause fluid accumulation in the lungs, which is characteristic of pulmonary oedema.
Option C is incorrect because asbestosis is a chronic lung disease caused by prolonged asbestos exposure, leading to scarring of lung tissue. It presents with progressive shortness of breath, but it does not cause acute symptoms or fine crackles at the lung bases in the manner seen with pulmonary oedema.
Option D is incorrect because viral respiratory infections generally cause symptoms such as fever, cough, and congestion. While they can lead to wheezing or crackles, they typically present with more upper respiratory symptoms and are less likely to cause the fine crackles seen in pulmonary oedema, which is due to fluid accumulation in the alveoli.
Option E is incorrect because foreign body aspiration would more likely present with unilateral wheezing or stridor, depending on the site of obstruction. It does not typically cause the fine crackles heard at the lung bases, which are a hallmark of fluid accumulation, as seen in pulmonary oedema.
Question 31:
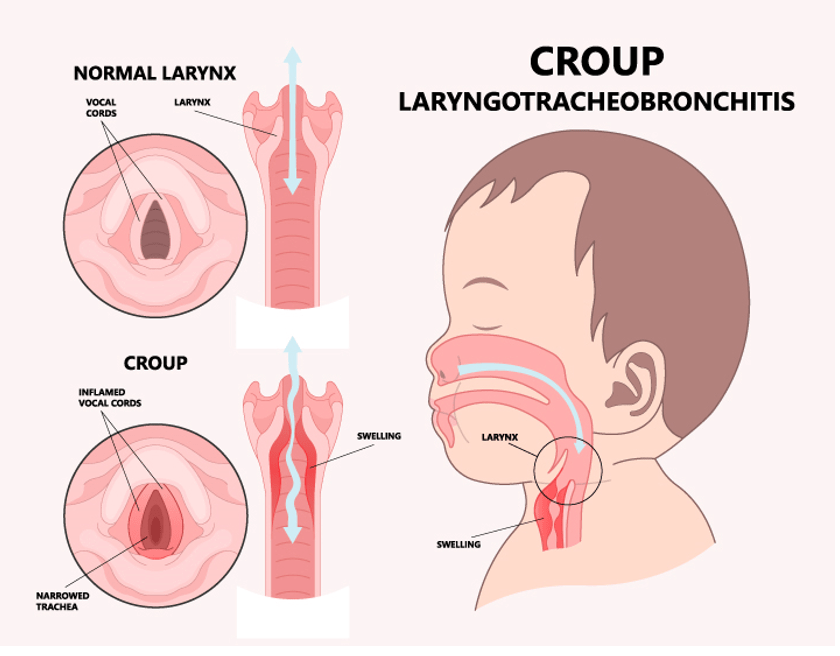
Answer: B) Croup (laryngotracheobronchitis)
Explanation:
This 2-year-old child presents with several key features that suggest croup:
- Sudden onset of barking cough: This is the classic hallmark of croup, which is caused by inflammation and swelling of the larynx and trachea.
- Stridor and hoarseness: These symptoms indicate upper airway obstruction, which is typical in croup due to swelling in the larynx and trachea.
- Mild fever: A low-grade fever is commonly seen in viral infections like croup, which is usually caused by parainfluenza virus.
- Symptoms worse at night: Croup symptoms tend to worsen at night due to increased airway inflammation and narrowing.
- Improvement with exposure to moist air: This is characteristic of croup, as the moist air helps to soothe the inflamed airways and reduce symptoms.
Option A is incorrect because acute epiglottitis typically presents with a high fever, severe respiratory distress, and difficulty swallowing. The child would often be sitting in a tripod position and have a much more urgent presentation. The barking cough and improvement with moist air do not fit the profile of acute epiglottitis.
Option C is incorrect because laryngomalacia is a congenital condition in which the soft tissues of the larynx collapse during inspiration, causing stridor. However, this condition is typically present from birth and causes chronic rather than sudden-onset symptoms. The improvement with moist air and the barking cough point to croup rather than laryngomalacia.
Option D is incorrect because foreign body aspiration usually presents with sudden-onset stridor and respiratory distress, often with a history of choking or inhaling a foreign object. It typically causes localised wheezing or stridor depending on the side of the obstruction and does not present with a barking cough or improve with exposure to moist air.
Option E is incorrect because bacterial tracheitis is a bacterial infection that can cause airway obstruction, but it typically presents with more severe symptoms, including high fever, significant respiratory distress, and purulent secretions. Tracheitis often presents with sharp stabbing pain in the sternum when coughing but does not cause the classic barking cough seen in croup and usually requires more aggressive treatment, such as antibiotics.
Question 32:
Answer: A) Bronchiolitis
Explanation:
This 3-year-old child presents with several key features that suggest bronchiolitis:
- Cough, mild wheezing, and crackles on auscultation: These symptoms are commonly seen in bronchiolitis, which is an inflammation of the small airways (bronchioles) typically caused by viral infections, such as Respiratory Syncytial Virus (RSV).
- Runny nose and slight fever: These are typical upper respiratory symptoms that often precede or accompany bronchiolitis, which usually starts as a viral upper respiratory infection before progressing to involve the lower airways.
- Not in severe respiratory distress: While bronchiolitis can cause respiratory symptoms, it typically presents with mild to moderate respiratory distress in children, especially in cases that do not require hospitalisation.
Option B is incorrect because tonsillitis usually presents with a sore throat, difficulty swallowing, and fever, rather than respiratory symptoms like wheezing, crackles, or cough. It would not cause wheezing or crackles on auscultation.
Option C is incorrect because pneumonia typically presents with more severe symptoms, such as high fever, tachypnoea, and significant respiratory distress. The child in this case has only mild symptoms and is not in severe distress. Pneumonia can also cause crackles, but it is usually associated with more pronounced respiratory difficulty.
Option D is incorrect because otitis media primarily presents with ear pain, fever, and sometimes irritability. While it can be associated with a respiratory infection, it would not cause wheezing, crackles, or significant cough.
Option E is incorrect because pneumonitis refers to inflammation of the lung tissue, often caused by an infection or exposure to harmful substances. It can cause symptoms similar to pneumonia but typically presents with more severe respiratory distress or a more significant history of exposure to toxins, which is not present in this case.

Question 33:
Answer: B) Respiratory Syncytial Virus (RSV)
Explanation:
This 2-year-old child presents with cough, wheezing, and mild respiratory distress, which are common symptoms of bronchiolitis. The most likely pathogen responsible for bronchiolitis in this age group is: Respiratory Syncytial Virus (RSV). RSV is the most common cause of bronchiolitis in infants and young children (especially in those under the age of 2). It leads to inflammation and congestion in the bronchioles, causing the characteristic wheezing, cough, and mild respiratory distress seen in this case.
Option A is incorrect because Streptococcus pneumoniae is a common cause of bacterial pneumonia, not bronchiolitis. While it can cause severe respiratory infections, it is not the primary cause of bronchiolitis in young children.
Option C is incorrect because Haemophilus influenzae is a bacterial pathogen that can cause infections such as pneumonia and epiglottitis. However, it is not the most common cause of bronchiolitis in children. RSV is the leading viral cause of bronchiolitis.
Option D is incorrect because the influenza virus can cause respiratory illness, including pneumonia, but it is not the most common cause of bronchiolitis. Influenza typically presents with more systemic symptoms, such as high fever and malaise, in addition to respiratory symptoms.
Option E is incorrect because Mycoplasma pneumoniae is a bacterial pathogen that causes atypical pneumonia, particularly in older children and adolescents. It does not cause bronchiolitis in young children and would not explain the wheezing and mild respiratory distress seen in this 2-year-old.
Question 34:
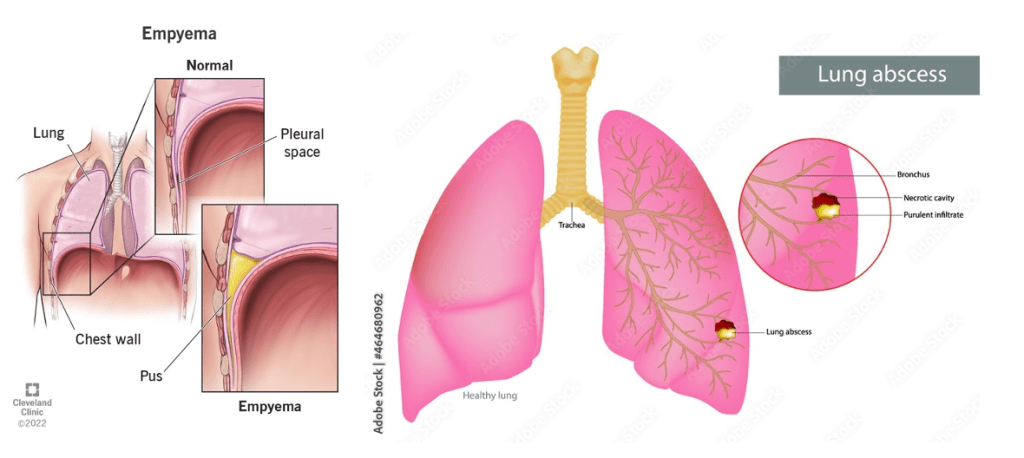
Answer: A) Lung abscess has a thick, walled cavity, while empyema presents with free-flowing pleural fluid
Explanation:
This 5-year-old child presents with fever, cough, pleuritic chest pain, and dullness to percussion with decreased breath sounds, suggesting a localised lung infection. Based on the diagnosis of a lung infection, the key difference between a lung abscess and empyema is: Lung abscess has a thick, walled cavity, which is a result of necrotic tissue and pus forming in the lung parenchyma. This forms a localised, encapsulated collection of infected material. Empyema is characterised by free-flowing pleural fluid in the pleural space, typically caused by a bacterial infection leading to an accumulation of pus in the pleural cavity. Unlike a lung abscess, empyema does not form a thick-walled cavity but involves fluid collection within the pleural space. The key difference is that in lung abscesses, pus forms accumulates in the lung parenchyma whereas in empyema, pus accumulates in pleural cavities.
Option B is incorrect because lung abscess is often associated with a consolidation or localised mass on chest X-ray, whereas empyema is associated with pleural fluid accumulation. Empyema would not be associated with a normal chest X-ray as it would show fluid or pleural effusion.
Option C is incorrect because while a lung abscess commonly occurs in the lower lobes, empyema can occur anywhere in the pleural space and is not specifically associated with the upper lobes. Empyema typically presents with pleural effusion, which can involve any area of the chest cavity.
Option D is incorrect because lung abscesses can result from both bacterial and anaerobic infections, not just viral infections, and empyema is usually caused by bacterial infections, particularly Streptococcus pneumoniae or Staphylococcus aureus.
Option E is incorrect because lung abscess presents with a localised fluid collection within the lung parenchyma, while empyema presents with fluid accumulation within the pleural space. Empyema involves pleural fluid, which can accumulate diffusely, but it is not characterised by a “localised” fluid collection like a lung abscess.
Question 35:
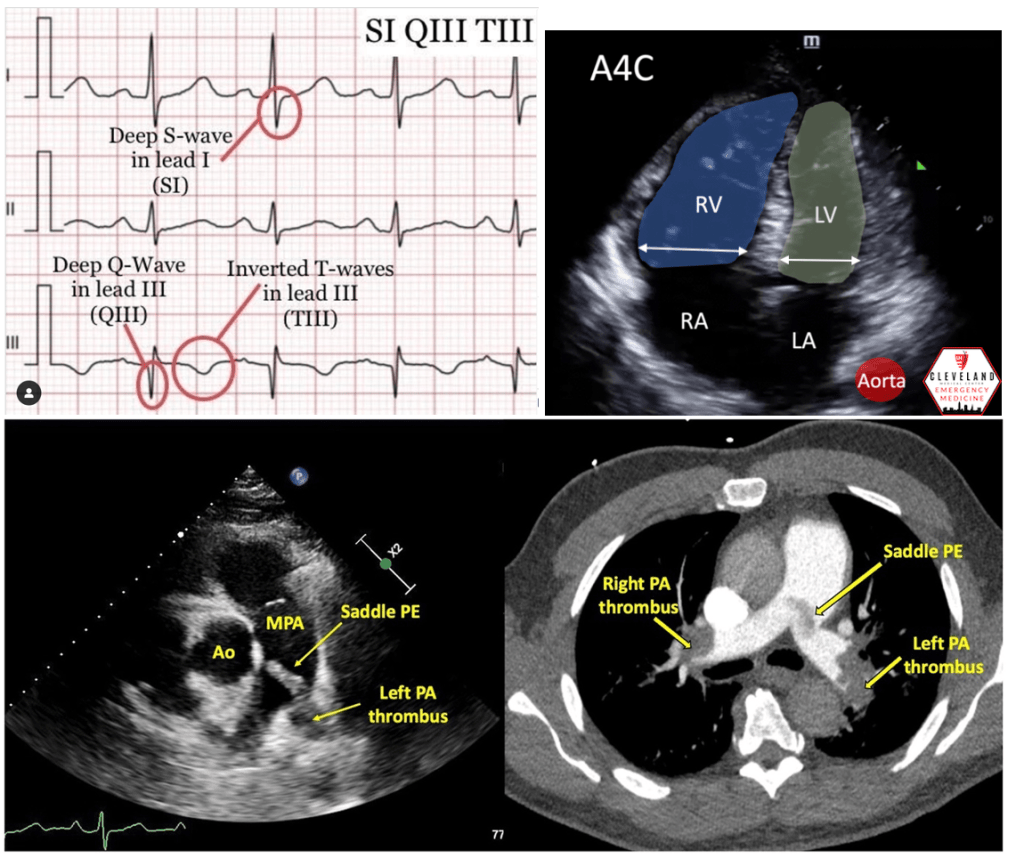
Answer: C) S1Q3T3 pattern on ECG
Explanation:
This 45-year-old man has a confirmed massive pulmonary embolism (PE) with clinical signs of right ventricular strain. The S1Q3T3 pattern on ECG is a hallmark finding associated with severe right ventricular strain caused by acute pressure overload.
• The S1Q3T3 pattern refers to the presence of a deep S wave in lead I, a Q wave in lead III, and an inverted T wave in lead III. This finding indicates right heart strain, commonly associated with massive or submassive PE.
• Right ventricular strain occurs when the right ventricle struggles to pump against the sudden increase in pulmonary artery pressure caused by the embolism.
Option A is incorrect because elevated D-dimer indicates the presence of clot degradation products but is not specific for right ventricular strain. Elevated D-dimer is commonly used to rule out PE in low-risk patients but does not directly measure the impact of the embolism on the right ventricle.
Option B is incorrect because a high-probability V/Q mismatch is a diagnostic finding of pulmonary embolism but does not indicate the severity of right ventricular strain. While a V/Q mismatch confirms PE, it does not provide information about the degree of strain on the heart.
Option D is incorrect because normal BNP (B-type natriuretic peptide) levels would be unlikely in severe right ventricular strain. Elevated BNP levels are often seen in conditions causing right ventricular overload, such as massive PE, and are a more typical finding in this context.
Option E is incorrect because a pulmonary artery (PA) width smaller than the aortic width on CT would suggest no significant pulmonary hypertension. In cases of massive PE with right ventricular strain, the PA is often dilated due to increased pulmonary pressure, so a smaller PA width compared to the aorta would not align with this diagnosis.
Question 36:
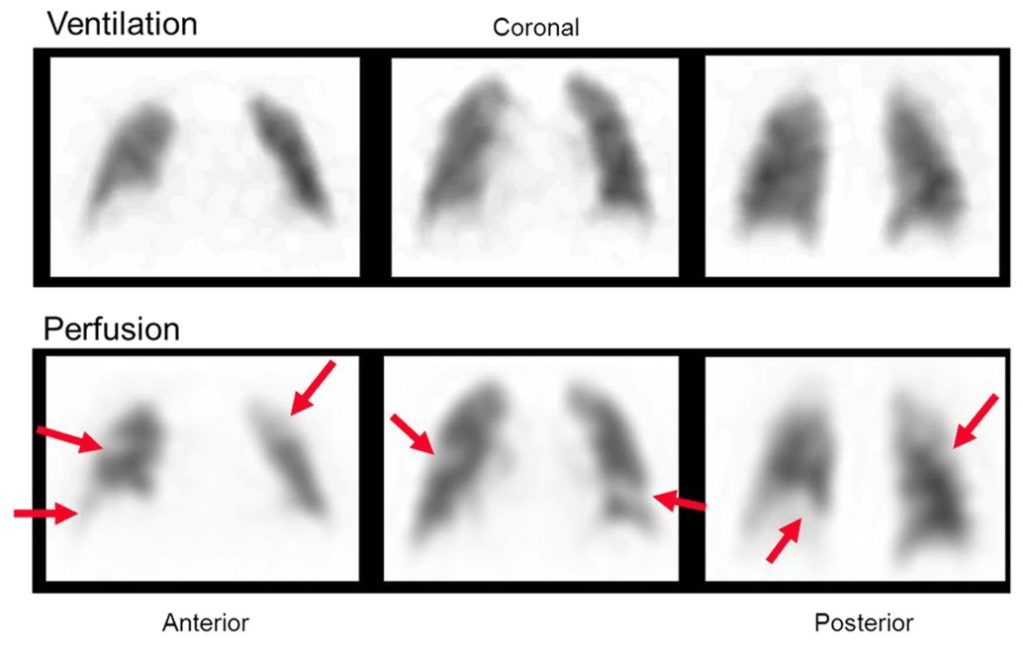
Answer: C) Mismatched ventilation/perfusion (V/Q) defect on a V/Q scan
Explanation:
A positive CT pulmonary angiogram (CTPA) usually provides a definitive diagnosis for a pulmonary embolism however the second best diagnostic method is a V/Q scan. A mismatched ventilation/perfusion (V/Q) defect on a V/Q scan is the most specific finding for diagnosing pulmonary embolism out of the following options.
• This refers to areas of the lung where ventilation is preserved but perfusion is impaired due to obstruction of pulmonary arteries by an embolus.
• The V/Q mismatch is a hallmark feature of PE, making it a highly specific diagnostic tool in certain clinical scenarios, especially when CT pulmonary angiography is unavailable or contraindicated e.g in pregnant women.
Option A is incorrect because elevated D-dimer is sensitive for the presence of clot formation but is not specific to pulmonary embolism. D-dimer levels can also be elevated in numerous other conditions, such as infection, cancer, or recent surgery, and therefore cannot confirm PE on their own. D-dimer is often used to rule out PE however a score of >500 indicates that there is a clot!
Option B is incorrect because Hampton’s Hump on chest X-ray, a wedge-shaped opacity representing pulmonary infarction, is a rare finding in PE. While it is suggestive of PE, it lacks sensitivity and specificity, as it may not be present in all cases.
Option D is incorrect because right axis deviation on ECG is a sign of right heart strain, which can occur in massive PE, but it is not specific to this condition. It can also be seen in other cardiac or pulmonary diseases, such as chronic obstructive pulmonary disease (COPD) or right ventricular hypertrophy.
Option E is incorrect because swelling, heat, and pain in the left leg are consistent with deep vein thrombosis (DVT), a common cause of PE, but these findings are not specific to PE. While DVT and PE are closely related, leg symptoms alone cannot confirm the presence of a pulmonary embolism.
Question 37:
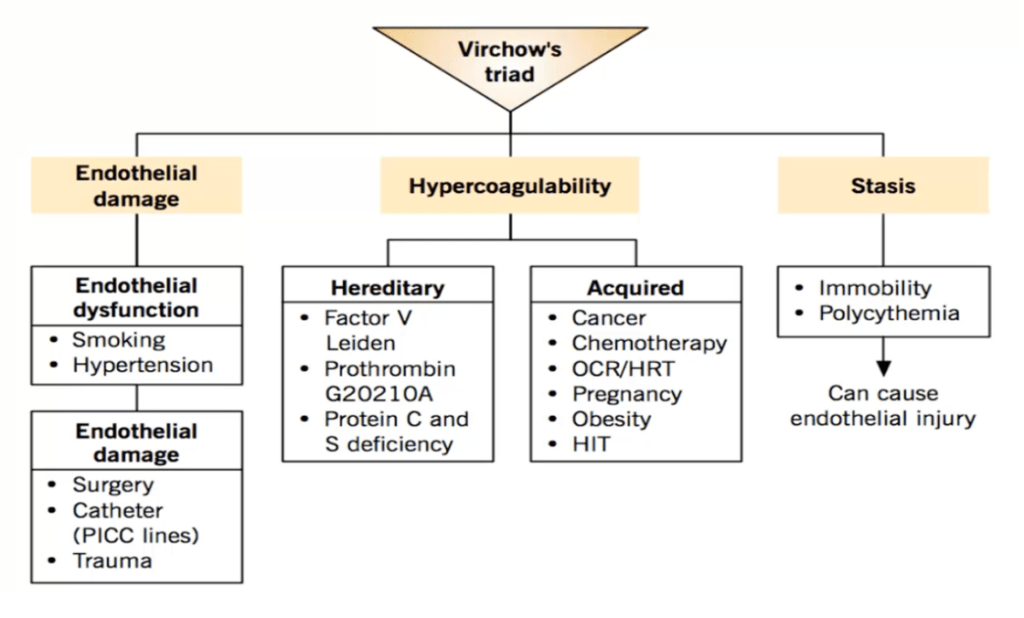
Answer: C) Stasis of blood flow
Explanation:
Stasis of blood flow is the most likely component of Virchow’s triad contributing to this patient’s condition.
• The patient’s recent abdominal surgery and prolonged immobility (bedridden for a week) have resulted in decreased blood flow in the veins of the legs.
• Stasis leads to pooling of blood, which increases the risk of clot formation, a key mechanism in the development of deep vein thrombosis (DVT).
Option A is incorrect because endothelial injury, another component of Virchow’s triad, typically occurs in conditions such as trauma, surgery directly affecting blood vessels, or inflammation of the vessel wall. While this patient underwent abdominal surgery, there is no direct evidence of endothelial injury in the veins of his left leg.
Option B is incorrect because hypercoagulability, another component of Virchow’s triad, can contribute to clot formation in patients with inherited thrombophilia, cancer, or certain medications like oral contraceptives. There is no indication in this patient’s history to suggest a hypercoagulable state.
Option D is incorrect because reduced oxygenation is not a component of Virchow’s triad. While it can exacerbate complications in conditions such as pulmonary embolism, it does not directly explain clot formation in the setting of DVT.
Option E is incorrect because vessel dilation is not a component of Virchow’s triad. It is typically associated with other vascular conditions like aneurysms or varicose veins, which are not implicated in this case.
Question 38:
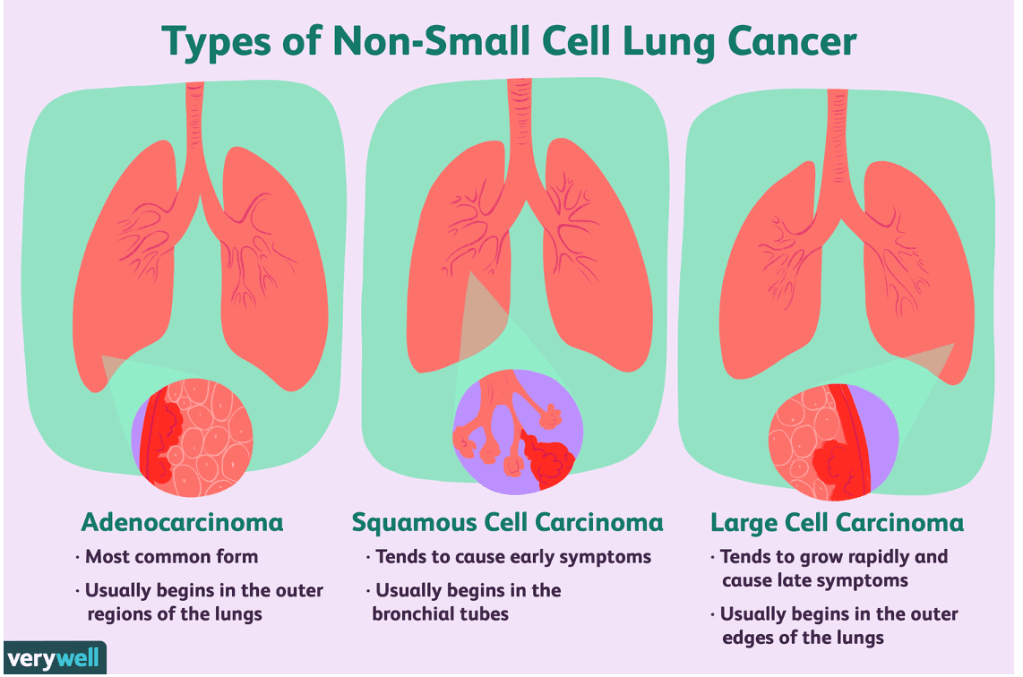
Answer: C) Squamous cell carcinoma
Explanation:
Squamous cell carcinoma is the most likely diagnosis in this patient due to the following features:
• Location of the tumour: Squamous cell carcinoma often arises centrally in the lung near the bronchi, consistent with the imaging findings of a central mass.
• Smoking history: A strong association exists between squamous cell carcinoma and smoking, and this patient has a significant 40-pack-year smoking history.
• Symptoms: Persistent cough, weight loss, and haemoptysis are common in centrally located lung cancers, including squamous cell carcinoma.
Option A is incorrect because small cell lung cancer is also strongly associated with smoking and arises centrally, but it is typically associated with rapid progression, paraneoplastic syndromes (e.g., SIADH or ectopic ACTH production), and more systemic symptoms. There is no mention of these findings in this case.
Option B is incorrect because adenocarcinoma is the most common type of lung cancer overall, particularly in non-smokers, and typically arises in the lung periphery rather than centrally. The patient’s central lung mass makes squamous cell carcinoma more likely.
Option D is incorrect because large cell carcinoma is a less common type of lung cancer that can occur peripherally or centrally. However, it does not have the same strong correlation with a central location near the bronchi and smoking history as squamous cell carcinoma does.
Option E is incorrect because mesothelioma is primarily associated with asbestos exposure and involves the pleura, presenting with pleural effusions or thickening, which are not mentioned in this case. A central lung mass is not typical of mesothelioma.
Question 39:
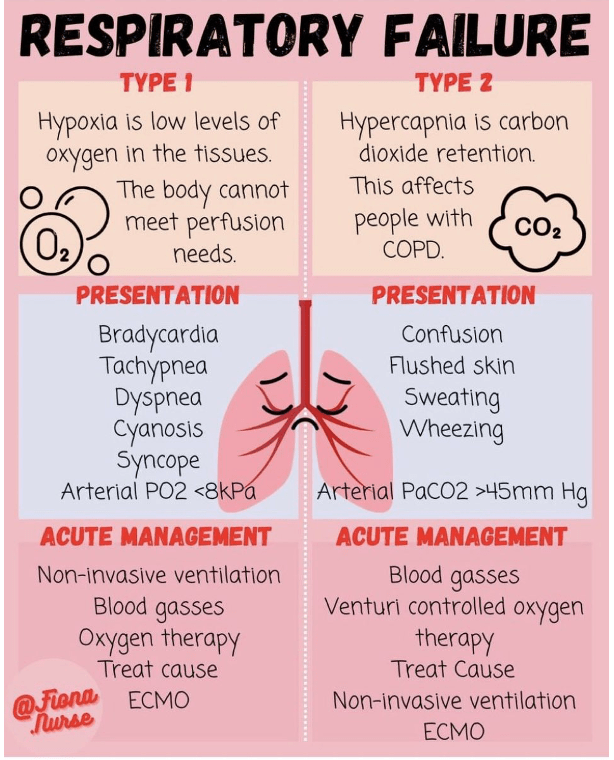
Answer: C) Acute Type 2 respiratory failure due to COPD exacerbation
Explanation:
This patient is most likely experiencing an acute exacerbation of COPD, leading to acute Type 2 respiratory failure. The following features support this diagnosis:
• Acid-base status on ABG: The pH of 7.31 (acidosis) and PaCO2 of 56 mmHg (hypercapnia) indicate respiratory acidosis, consistent with Type 2 respiratory failure. The acute nature of the acidosis is suggested by the pH being below normal, showing the body has not fully compensated.
• Worsening symptoms: The patient has worsening shortness of breath and tachypnoea, which are typical of an acute exacerbation of COPD.
• Chest X-ray findings: Hyperinflated lungs are a classic finding in COPD, and the absence of other abnormalities like pneumonia or pneumothorax makes exacerbation of COPD the likely cause.
• Oxygenation: His PaO2 of 50 mmHg indicates hypoxaemia, which is consistent with COPD exacerbation causing ventilation-perfusion mismatch.
Option A is incorrect because Type 1 respiratory failure involves hypoxaemia (PaO2 < 60 mmHg) without hypercapnia, which is not the case here. Diffuse alveolar damage would be seen in acute respiratory distress syndrome (ARDS), which is not supported by the history or chest X-ray findings.
Option B is incorrect because chronic Type 2 respiratory failure occurs in patients with baseline hypercapnia and respiratory acidosis that is well-compensated over time. This patient’s worsening symptoms, decompensated pH, and acute presentation point to an acute cause rather than a chronic steady state.
Option D is incorrect because pulmonary embolism typically causes Type 1 respiratory failure due to impaired oxygenation (V/Q mismatch), not Type 2 respiratory failure with hypercapnia. Additionally, no features like pleuritic chest pain, haemoptysis, or risk factors for thromboembolism are mentioned.
Option E is incorrect because Type 2 respiratory failure due to chest wall deformity would be a chronic condition, typically associated with long-standing restrictive lung disease rather than an acute exacerbation. This patient has a clear history of COPD, which is more relevant to the presentation.
Question 40:
Answer: C) Epiglottitis
Explanation:
This 6-year-old child presents with classic signs and symptoms of epiglottitis, which include:
• Fever, drooling, and stridor: These are hallmark symptoms of epiglottitis. The stridor is typically high-pitched and worse with inspiration due to airway obstruction.
• Inability to swallow saliva: This indicates severe inflammation and swelling of the epiglottis, leading to dysphagia.
• Toxic appearance: The child appears acutely unwell, which is characteristic of epiglottitis, a potentially life-threatening condition.
• Absence of cough: Unlike croup, which is associated with a barking cough, epiglottitis does not typically present with a cough.
• Respiratory distress: The child is visibly struggling to breathe, as evidenced by the high-pitched stridor and inability to manage secretions.
Option A is incorrect because croup typically presents with a barking cough, hoarseness, and stridor, which is usually less severe than the stridor seen in epiglottitis. Moreover, croup does not typically cause drooling or an inability to swallow saliva, and children with croup do not appear toxic.
Option B is incorrect because tonsillitis, while causing fever and difficulty swallowing, does not usually lead to stridor or respiratory distress. Additionally, tonsillitis typically presents with sore throat and swollen tonsils, which are not mentioned in this case.
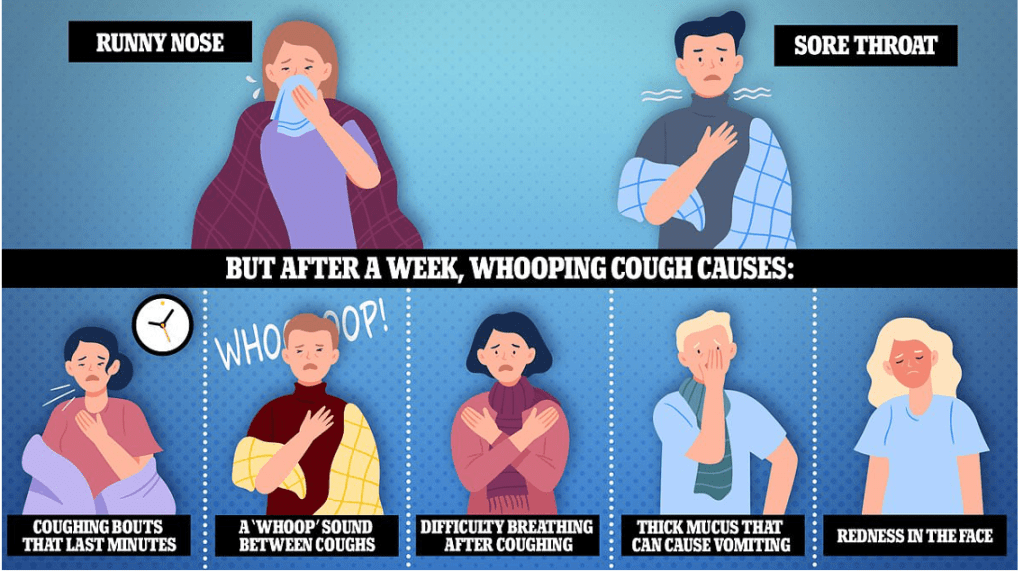
Option D is incorrect because pertussis (whooping cough) causes paroxysmal coughing fits with inspiratory “whooping” sounds, which is not described in this child. Pertussis is less likely in a vaccinated child.
Option E is incorrect because the common cold causes mild upper respiratory symptoms like runny nose, cough, and mild fever. It does not cause stridor, drooling, or respiratory distress, and children with the common cold do not appear toxic.
Question 41:
Answer: C) Pertussis
Explanation:
This 6-year-old child presents with features that are characteristic of pertussis (whooping cough), which include:
• Persistent dry cough: Pertussis is marked by paroxysmal coughing fits that can last for weeks.
• Vomiting after coughing episodes: Post-tussive emesis is a classic symptom of pertussis.
• Cyanosis and apnoea: Severe coughing fits can lead to temporary cyanosis and apnoea due to decreased oxygenation.
• Facial flush: This occurs during prolonged bouts of coughing due to increased intrathoracic pressure.
Option A is incorrect because epiglottitis typically presents with fever, drooling, stridor, and a toxic appearance. It is an acute condition, unlike the prolonged coughing fits described here.
Option B is incorrect because croup usually presents with a barking cough, hoarseness, and inspiratory stridor, none of which are described in this case.
Option D is incorrect because tonsillitis typically presents with fever, sore throat, and difficulty swallowing, often with visible swollen tonsils. It does not cause the paroxysmal coughing or post-tussive vomiting seen in pertussis.
Option E is incorrect because the common cold is a mild viral illness with symptoms such as runny nose, congestion, and occasional mild cough. It does not cause severe coughing fits, cyanosis, or apnoea.
Question 42:
Answer: B) Dexamethasone
Explanation:
This 3-year-old child presents with symptoms consistent with croup (laryngotracheobronchitis), which include:
• Barking cough: This is a hallmark symptom of croup, caused by inflammation of the upper airway.
• Inspiratory stridor: Indicates airway obstruction due to narrowing of the subglottic region.
• Difficulty breathing, especially at night: Symptoms of croup tend to worsen at night.
• Recent viral upper respiratory tract infection: Croup is typically caused by parainfluenza viruses.
The first-line treatment for croup is dexamethasone, a corticosteroid that reduces airway inflammation, improves symptoms, and decreases the need for further interventions.
Option A is incorrect because macrolides are antibiotics used for bacterial infections such as Bortadella Pertussis, not for croup, which is viral in origin.
Option C is incorrect because antibiotics are not indicated for croup, as it is usually caused by a viral infection.
Option D is incorrect because intubation is a last-resort intervention reserved for severe cases of croup with impending respiratory failure, which is not described in this scenario.
Option E is incorrect because antivirals are not effective for parainfluenza or the other common viruses that cause croup. Antivirals are more specific to conditions like influenza or herpesvirus infections.
Question 43:
Answer: B) Bronchiolitis
Explanation:
This 9-month-old infant presents with clinical features characteristic of bronchiolitis, which include:
• Increasing respiratory distress: Manifested by nasal flare, tracheal tug, and intercostal retractions, indicating significant effort to breathe.
• Recent upper respiratory tract symptoms: A runny nose and cough are typical early signs of bronchiolitis.
• Poor feeding: Suggests worsening respiratory compromise and fatigue.
• Crackles and wheezing: These are hallmark auscultatory findings in bronchiolitis due to inflammation and obstruction of small airways.
Bronchiolitis is most commonly caused by respiratory syncytial virus (RSV) and typically affects infants and young children under 2 years of age.
Option A is incorrect because pneumonia often presents with focal consolidation or lobar findings on auscultation and typically involves higher fever and more severe systemic symptoms compared to bronchiolitis.
Option C is incorrect because measles presents with a distinct rash, Koplik spots, and systemic symptoms such as high fever, which are not described in this case.
Option D is incorrect because influenza is characterised by systemic symptoms such as high fever, myalgia, and malaise, and does not commonly present with crackles or wheezing in this age group.
Option E is incorrect because bronchiectasis is a chronic condition with recurrent infections, persistent productive cough, and does not typically present acutely in a previously healthy infant.
Question 44:
Answer: B) Start empiric antibiotic therapy
Explanation:
This 3-year-old child presents with a high fever, cough, difficulty breathing, tachypnoea, tachycardia, and decreased breath sounds with crackles on auscultation. These findings are concerning for a lower respiratory tract infection, such as bacterial pneumonia. In clinical practice, starting empiric antibiotic therapy such as 40-50 mg/kg of Amoxicillin is often the first step when a bacterial infection is suspected, especially in a child with these symptoms, to cover common pathogens like Streptococcus pneumoniae or Haemophilus influenzae.
Option A is incorrect because a throat swab for PCR testing would be more useful for diagnosing viral infections like influenza or RSV, but in this case, the clinical presentation is more suggestive of bacterial pneumonia, which should be addressed first with antibiotics.
Option C is incorrect because while a chest X-ray (CXR) is helpful in confirming pneumonia, in the UK, it is typically not ordered immediately in cases of suspected bacterial pneumonia unless there is a failure to improve after 48 hours of antibiotic therapy or if there are severe complications. Empiric antibiotic therapy should be initiated first.
Option D is incorrect because obtaining a blood culture is important to identify any bloodstream infections, but it is not the first step in diagnosis. In this case, empiric antibiotics are prioritised to treat the suspected bacterial infection while awaiting further diagnostic results.
Option E is incorrect because a complete blood count (CBC) can help assess infection or inflammation, but it is not diagnostic. The priority is to treat the child with empiric antibiotics, especially when bacterial pneumonia is suspected based on the clinical presentation.
Question 45:
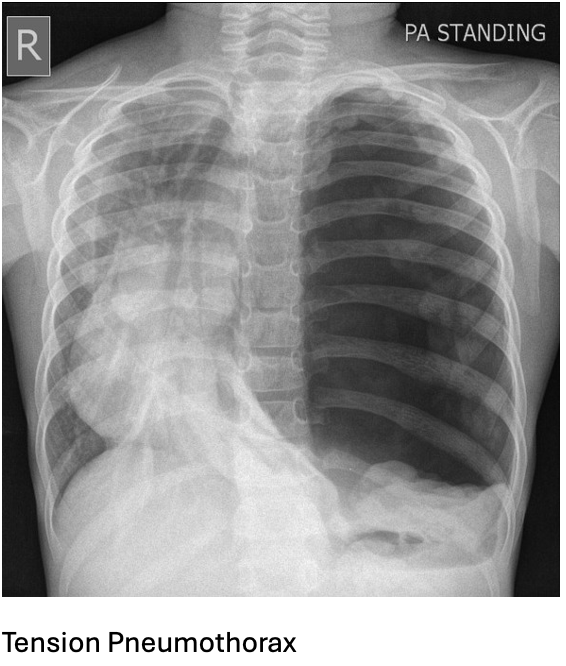
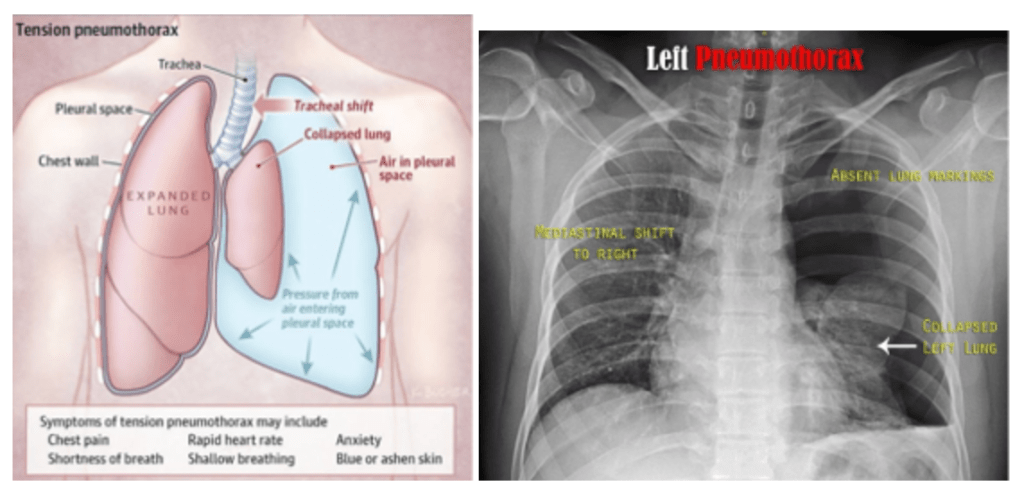
Answer: B) Tension pneumothorax – Needle decompression
Explanation:
This 35-year-old male presents with chest trauma and signs of respiratory distress, including decreased breath sounds on the left side, tracheal deviation to the right, and distended jugular veins. These clinical signs suggest a tension pneumothorax, a life-threatening condition where air is trapped in the pleural space, increasing pressure, and causing a shift of mediastinal structures (such as the trachea) to the opposite side. The immediate intervention for tension pneumothorax is needle decompression to relieve the pressure and prevent further deterioration.
Option A is incorrect because although an open pneumothorax (also known as a sucking chest wound) can cause similar symptoms, it is not characterised by tracheal deviation or distended jugular veins. The immediate treatment for open pneumothorax would be to apply a chest seal to prevent air from entering the pleural space.
Option C is incorrect because while a massive haemothorax (large amount of blood in the pleural cavity) can cause similar respiratory distress and decreased breath sounds, the key finding in this case is the tracheal deviation and distended jugular veins, which are more typical of tension pneumothorax. The immediate treatment for haemothorax is the insertion of a chest tube.
Option D is incorrect because flail chest (multiple rib fractures leading to a segment of the chest wall moving independently) can cause respiratory distress, but it does not typically cause tracheal deviation or distended jugular veins. The treatment for flail chest is to provide pain management, support ventilation & secure ribs using metal plates.
Option E is incorrect because cardiac tamponade (fluid accumulation in the pericardial sac) can cause distended jugular veins and respiratory distress, but it would not typically present with tracheal deviation to the opposite side of the fluid accumulation. The treatment for tamponade is pericardiocentesis, but the patient’s presentation is more consistent with a tension pneumothorax.
Question 46:
Answer: C) Observation and oxygen therapy
Explanation:
This 30-year-old male presents with a small left-sided pneumothorax following blunt chest trauma. He has sharp chest pain, difficulty breathing, and hyperresonance on percussion over the left lung, which is typical of a pneumothorax. His vital signs (respiratory rate of 30 breaths per minute) and examination findings suggest a small, uncomplicated pneumothorax. In this case, the most appropriate management is observation and oxygen therapy, as small pneumothoraxes (typically less than 2 cm on chest X-ray) often resolve on their own. Oxygen therapy helps to reabsorb the trapped air more quickly.
Option A is incorrect because chest tube placement is generally reserved for larger pneumothoraxes, those causing respiratory distress, or those that do not resolve with observation. This patient has a small, uncomplicated pneumothorax, so chest tube placement is not immediately necessary.
Option B is incorrect because needle thoracostomy is typically performed for tension pneumothorax, where there is severe respiratory distress, tracheal deviation, and hemodynamic instability. This patient does not have signs of tension pneumothorax, making needle thoracostomy unnecessary at this stage.
Option D is incorrect because thoracotomy is a surgical procedure typically indicated for severe trauma, massive haemothorax, or cases where a large pneumothorax or persistent air leak cannot be managed with less invasive techniques. This patient’s pneumothorax is small and does not require such an invasive procedure.
Option E is incorrect because pericardiocentesis is performed to treat cardiac tamponade, a condition where fluid accumulates in the pericardium, compressing the heart. This patient’s presentation is more consistent with a pneumothorax, not cardiac tamponade, so pericardiocentesis is not appropriate.
Question 47:
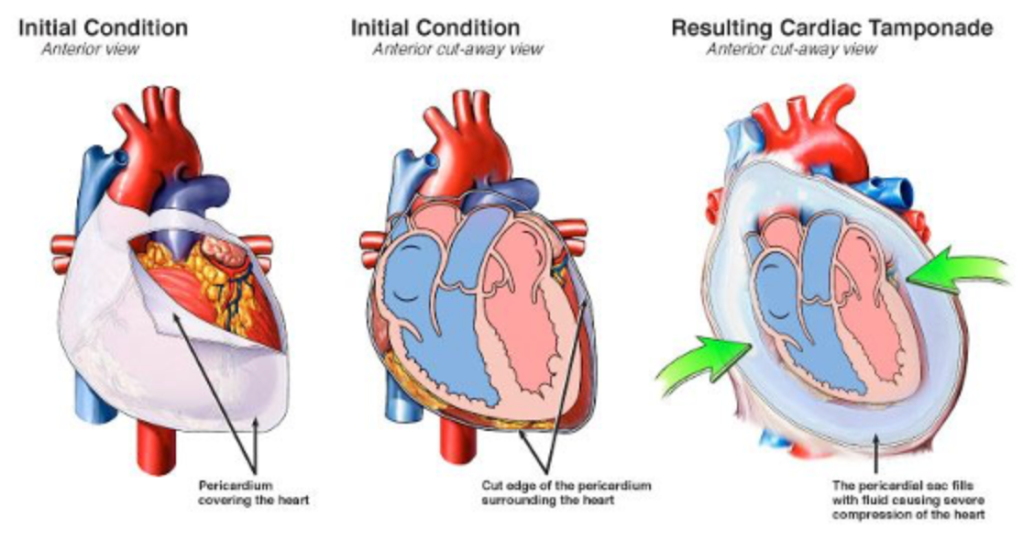
Answer: A) Cardiac tamponade due to traumatic pericardial effusion – Immediate pericardiocentesis
Explanation:
This 45-year-old male presents with signs and symptoms suggestive of cardiac tamponade, including severe respiratory distress, hypotension (90/60 mmHg), tachycardia (120 bpm), tachypnoea, and distended neck veins. He also exhibits muffled heart sounds and a paradoxical decrease in systolic blood pressure with inspiration (pulsus paradoxus), which are hallmark signs of cardiac tamponade. The bedside echocardiogram revealing an effusion surrounding the heart with early signs of right atrial collapse further supports this diagnosis. In this scenario, the most appropriate next step is immediate pericardiocentesis to relieve the pressure around the heart and restore normal cardiac function. The patient has the characteristic features of Beck’s triad!!!
Option B is incorrect because cardiac tamponade due to acute myocardial infarction typically presents with a history of chest pain and signs of myocardial injury, such as elevated troponin levels, but this patient’s clinical presentation is more consistent with traumatic pericardial effusion due to a high-speed collision. Emergent coronary angiography is not the first step in this case.
Option C is incorrect because tension pneumothorax presents with severe respiratory distress, tracheal deviation, and absent breath sounds on one side of the chest. Although this patient is tachypnoeic and hypotensive, the absence of signs such as tracheal deviation, hyperresonance on percussion, and absent breath sounds makes tension pneumothorax less likely. The bedside echocardiogram also does not suggest a pneumothorax, making needle thoracostomy unnecessary.
Option D is incorrect because massive haemothorax typically presents with signs of blood loss (hypotension, tachycardia) and dullness to percussion on the affected side. While this patient is hypotensive and tachycardic, the chest X-ray does not show evidence of a massive haemothorax, and the primary issue appears to be related to a pericardial effusion, not blood in the pleural space.
Option E is incorrect because pulmonary embolism presents with sudden onset of pleuritic chest pain, dyspnoea, and sometimes haemoptysis. It typically does not cause muffled heart sounds or pulsus paradoxus, which are specific to cardiac tamponade. Additionally, the bedside echocardiogram findings are more consistent with tamponade, not a pulmonary embolism, making anticoagulation inappropriate in this scenario.
Question 48:
Answer: C) Bruising of the lung tissue leading to oedema and haemorrhage
Explanation:
This patient presents with blunt chest trauma and a chest X-ray revealing patchy infiltrates without obvious fractures. The most likely diagnosis in this case is pulmonary contusion, which occurs due to direct injury to the lung tissue. Pulmonary contusion leads to bruising of the lung, causing oedema and haemorrhage within the lung parenchyma. This results in the appearance of patchy infiltrates on the chest X-ray, which is characteristic of this condition. Pulmonary contusions can occur after blunt trauma and may worsen over time, often causing respiratory distress due to impaired gas exchange.
Option A is incorrect because disruption of the pleura leading to air in the pleural space results in a pneumothorax. While pneumothorax can be a consequence of chest trauma, it would typically present with more distinct clinical findings, such as decreased breath sounds and hyperresonance on percussion, which are not mentioned in this case.
Option B is incorrect because accumulation of blood in the pleural space results in a haemothorax, which is typically seen with more severe trauma and would present with dullness to percussion on the affected side. The X-ray finding of patchy infiltrates without evidence of pleural fluid makes haemothorax less likely.
Option D is incorrect because rupture of the trachea or bronchial tree can lead to subcutaneous emphysema, mediastinal emphysema, or pneumothorax, which would be more apparent on a chest X-ray, particularly with evidence of air outside the lung or within the mediastinum. There is no mention of such findings in this case.
Option E is incorrect because compression of the heart by fluid accumulation in the pericardium results in cardiac tamponade, which would present with symptoms such as hypotension, jugular venous distension, and muffled heart sounds, not with patchy infiltrates on a chest X-ray. This condition would also not be caused by blunt chest trauma in the absence of other findings.
Question 49:
Answer: B) Subcutaneous emphysema – chest drain
Explanation:
This patient presents with chest trauma, difficulty breathing, and subcutaneous crepitus (described as a “bubble wrap” sensation) in the upper chest, face, and neck. These findings are characteristic of subcutaneous emphysema, which occurs when air escapes from the lungs or airways into the subcutaneous tissues. The most common cause in the setting of chest trauma is pneumothorax, particularly if the pleura or lung parenchyma has been disrupted. A chest X-ray or CT scan is typically performed to confirm the presence of a pneumothorax.
The treatment for subcutaneous emphysema involves addressing the underlying cause, which is most commonly a pneumothorax. The insertion of a chest drain (thoracostomy) allows air to escape from the pleural cavity, reducing pressure and preventing further air leakage into the subcutaneous tissue.
Option A is incorrect because tension pneumothorax is a life-threatening condition where air accumulates in the pleural space under pressure, leading to tracheal deviation, hypotension, and respiratory distress. While a chest drain is part of the treatment for tension pneumothorax, the absence of these findings in this case makes it unlikely.
Option C is incorrect because flail chest involves fractures of multiple adjacent ribs in multiple places, leading to paradoxical chest wall movement. There is no mention of chest wall instability or rib fractures in this case.
Option D is incorrect because pulmonary contusion results from bruising of lung tissue, causing oedema and haemorrhage. While it can occur in chest trauma, it does not explain the subcutaneous crepitus described in this patient.
Option E is incorrect because haemothorax involves blood accumulation in the pleural space, which typically presents with signs such as decreased breath sounds and dullness to percussion. It would not cause subcutaneous emphysema.
Question 50:
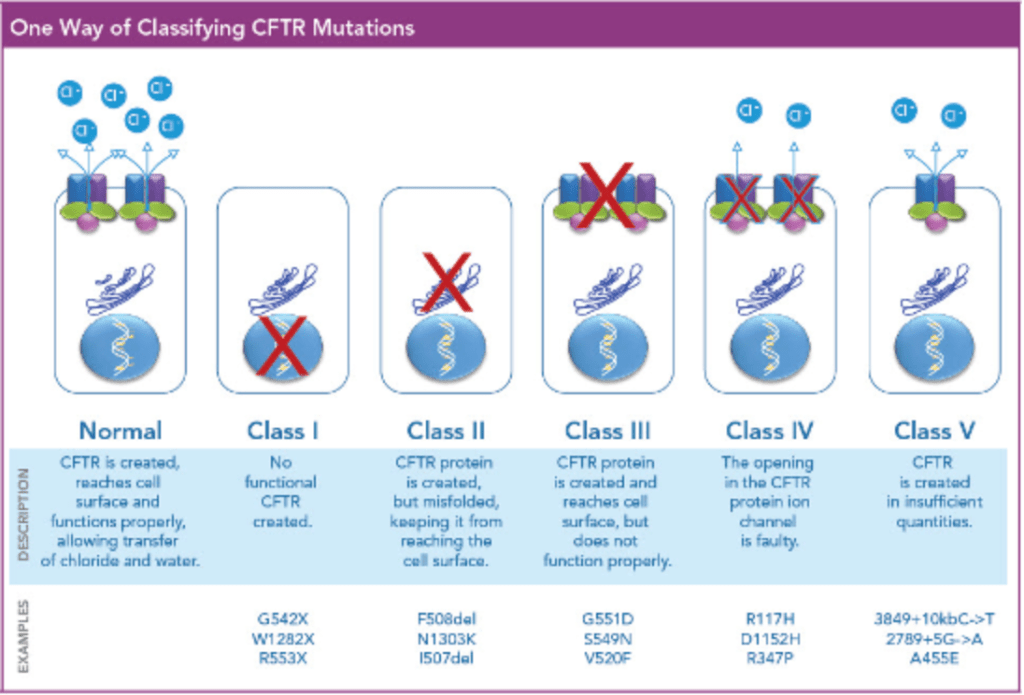
Answer: B) Class II – No traffic (mis-shaped protein)
Explanation:
This 5-year-old child presents with recurrent respiratory infections, chronic cough, nasal polyps, poor growth despite a good appetite, and persistently high immune-reactive trypsinogen on newborn screening. These findings are highly suggestive of cystic fibrosis (CF). CF is caused by mutations in the CFTR (cystic fibrosis transmembrane conductance regulator) gene, which encodes a chloride channel.
Class II mutations, such as the common F508del mutation, result in the production of a misfolded CFTR protein that cannot traffic to the cell surface, leading to defective chloride transport. This accounts for the majority of CF cases worldwide.
Option A is incorrect because Class I mutations involve a non-functional protein due to premature stop codons or frameshift mutations, leading to an absence of CFTR protein. These mutations also cause CF, but the clinical scenario described here most commonly involves a Class II mutation.
Option C is incorrect because Class III mutations reduce CFTR gating, meaning that the protein reaches the cell surface but has impaired function. Examples include the G551D mutation.
Option D is incorrect because Class IV mutations decrease ion conduction through the CFTR channel. These mutations tend to cause a milder phenotype compared to Class II mutations.
Option E is incorrect because Class V mutations reduce the synthesis of CFTR protein but do not completely abolish its function. These mutations are also associated with a milder clinical presentation.
Question 51:
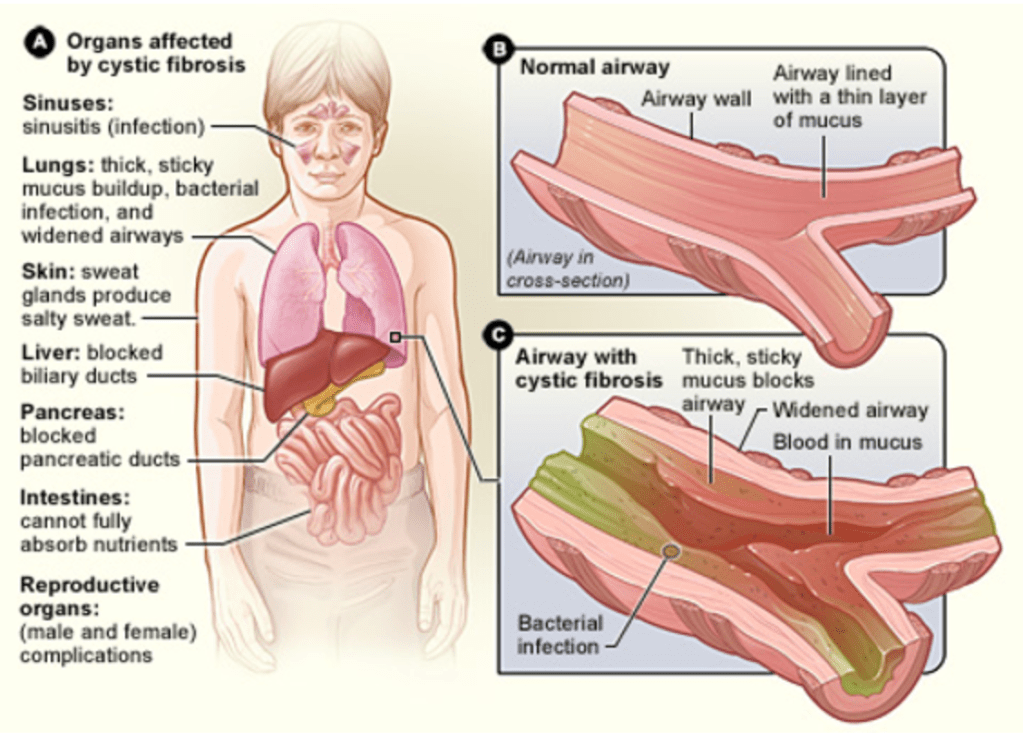
Answer: A) Impaired chloride secretion leading to dehydrated mucus and airway obstruction
Explanation:
This 12-year-old boy with cystic fibrosis (CF) presents with classic features of the disease, including chronic cough, increased sputum production, recurrent respiratory infections, sinusitis, nasal polyps, and a barrel chest. The primary pathophysiological mechanism in CF is impaired chloride secretion due to CFTR dysfunction. This leads to reduced water movement into the airway lumen, resulting in dehydrated and thickened mucus. The thick mucus obstructs the airways, provides a breeding ground for bacterial infections, and contributes to chronic inflammation and progressive lung damage.
Option B is incorrect because, while sodium absorption is increased in CF airways, the primary issue is impaired chloride secretion, which disrupts the ionic balance and causes mucus dehydration.
Option C is incorrect because dysfunctional ciliary action can occur secondarily due to thickened mucus in CF, but it is not the primary pathophysiological mechanism of the disease.
Option D is incorrect because bronchial smooth muscle constriction is more characteristic of asthma, not CF. The airway obstruction in CF is due to thickened mucus rather than smooth muscle constriction.
Option E is incorrect because reduced pulmonary vascular permeability leading to interstitial oedema is not a feature of CF. CF-related lung disease primarily involves mucus obstruction, infection, and inflammation, rather than vascular issues.
Question 52:
Answer: B) Pneumocystis Jirovecii
Explanation:
This 35-year-old woman with a history of immunosuppression due to a kidney transplant presents with classic signs of Pneumocystis jirovecii pneumonia (PJP). Key features include dyspnoea, fever, hypoxia, diffuse crackles, and bilateral infiltrates on chest X-ray. PJP is a common opportunistic infection in immunosuppressed patients, such as those on chronic immunosuppressive therapy or with HIV/AIDS. The identification of yeast-like organisms in her sputum supports this diagnosis.
Option A is incorrect because Mycobacterium tuberculosis typically causes localised cavitary lesions or consolidations in the lungs, and its presentation is usually more insidious than the acute course described here.
Option C is incorrect because Streptococcus pneumoniae typically causes lobar pneumonia rather than diffuse bilateral infiltrates. Moreover, bacterial pneumonia generally improves with antibiotics, whereas this patient’s condition deteriorated.
Option D is incorrect because Paragonimus Westermani, a parasitic lung fluke not fungi, is rare and associated with eating undercooked crustaceans. It typically causes haemoptysis and localised pulmonary findings rather than diffuse infiltrates.
Option E is incorrect because Echinococcus granulosus causes hydatid cysts (parasite not fungi), which appear as well-defined masses on imaging rather than diffuse infiltrates. It is also less likely in this clinical setting. It is transferred from sheep to dogs, & from dogs to human e.g. by kissing a dog.
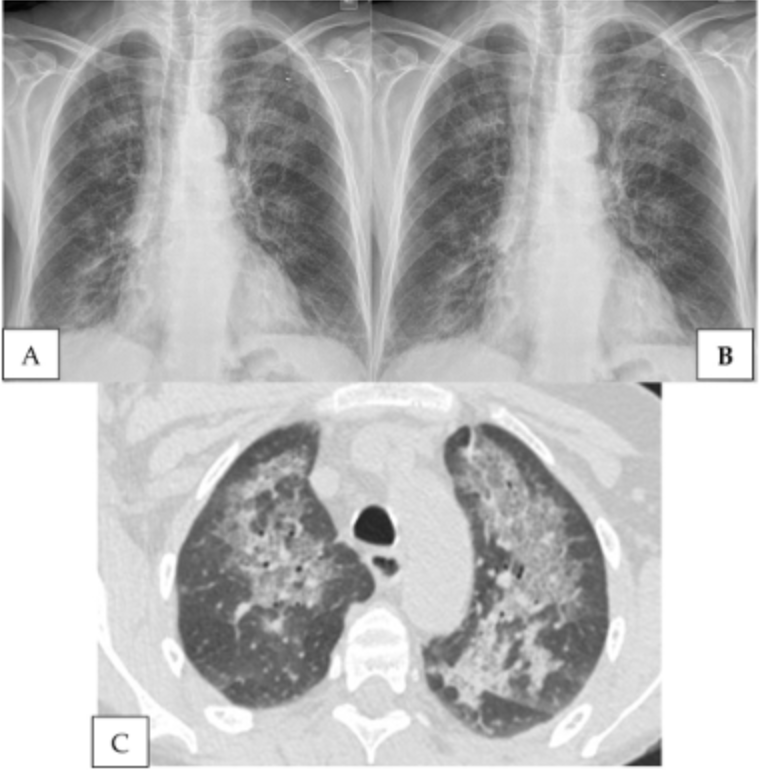
Question 53:
Answer: C) Initiate TB treatment with Isoniazid, Rifampin, Pyrazinamide, and Ethambutol and admit the patient for isolation.
Explanation:
This 45-year-old man with HIV presents with clinical features highly suggestive of active pulmonary tuberculosis (TB), including chronic cough, night sweats, weight loss, and a positive Mantoux test. The chest X-ray findings and immunosuppressed state due to HIV further support this diagnosis. Immediate initiation of a four-drug anti-TB regimen (Isoniazid, Rifampin, Pyrazinamide, and Ethambutol) is the appropriate first step, and the patient should be admitted for isolation to prevent the spread of TB. Isoniazid & Rifampin should be given for a full 6 months whereas Pyrazinamide & Ethambutol should only be prescribed for the first 6 months.
Option A is incorrect because while both TB treatment and antiretroviral therapy (ART) are crucial in managing HIV-associated TB, ART should generally be delayed for 2–8 weeks after starting TB therapy to avoid immune reconstitution inflammatory syndrome (IRIS), especially in patients with advanced HIV disease.
Option B is incorrect because a full four-drug regimen is needed to treat TB initially, not just Isoniazid and Rifampin. ART should also not be deferred until TB treatment is completed, as managing both conditions concurrently is critical.
Option D is incorrect because surgical removal of lung consolidation is not a standard treatment for pulmonary TB. Pharmacologic therapy with anti-TB drugs is the cornerstone of management.
Option E is incorrect because the clinical presentation strongly suggests TB, not community-acquired pneumonia. Empiric antibiotics for bacterial pneumonia would not address the underlying issue, delaying appropriate treatment.
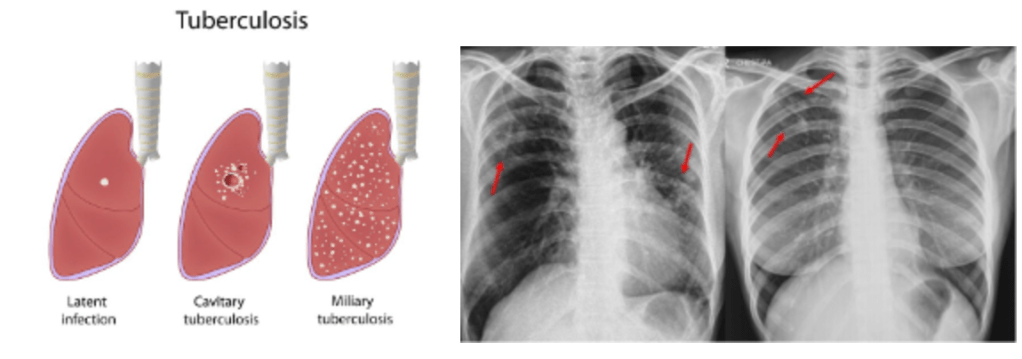
Question 54:
Answer: A) The 23-valent polysaccharide vaccine is recommended because he is older than 65 years.
Explanation:
In the UK, the pneumococcal vaccination schedule specifies that the 23-valent polysaccharide vaccine (PPSV23) is recommended for all adults aged 65 years and older. This vaccine is effective in preventing invasive pneumococcal disease in adults and is also routinely given to individuals with chronic conditions like COPD or immunocompromised patients.
The 13-valent conjugate vaccine (PCV13) is generally reserved for use in children as part of the routine immunisation schedule. It is not part of the standard vaccination schedule for healthy adults or those with COPD in the UK.
Option B is incorrect because PCV13 is primarily used in children.
Option C is incorrect because routine administration of both PCV13 and PPSV23 is not indicated for older adults.
Option D is incorrect because PCV13 only protects against invasive disease not localised pneumonia, but it is not routinely recommended for adults in this age group.
Option E is incorrect because pneumococcal vaccination is specifically indicated for older adults and those with chronic diseases like COPD to reduce the risk of pneumococcal infections.
Question 55:
Answer: E) Rheumatoid Arthritis-associated Interstitial Lung Disease – ILD associated with autoimmune disease
Explanation:
The patient has a history of rheumatoid arthritis (RA) and presents with symptoms of interstitial lung disease (ILD), including progressive dry cough, shortness of breath, and fine inspiratory crackles on physical exam. A high-resolution CT scan showing honeycombing at the lung bases is a characteristic finding of ILD. Given his RA and the use of methotrexate, the most likely cause of his ILD is rheumatoid arthritis-associated interstitial lung disease. ILD can occur in patients with RA, and this condition is often progressive.
Option A is incorrect because idiopathic pulmonary fibrosis (IPF) is a primary fibrotic lung disease without an identifiable cause, and it is not associated with rheumatoid arthritis.
Option C is incorrect because methotrexate-induced pneumonitis typically presents with acute or subacute symptoms, and while it can cause lung injury, the patient’s history and imaging findings point more toward rheumatoid arthritis-associated ILD rather than a drug-induced pneumonitis.
Option D is incorrect because sarcoidosis is a granulomatous disease and usually presents with bilateral hilar lymphadenopathy, which is not described in this patient’s case. The cause of sarcoidosis is generally unknown too, but it is thought to be due to an inhaled substance.
Option E is incorrect because asbestosis is associated with exposure to asbestos fibres, and there is no mention of such exposure in the patient’s history.
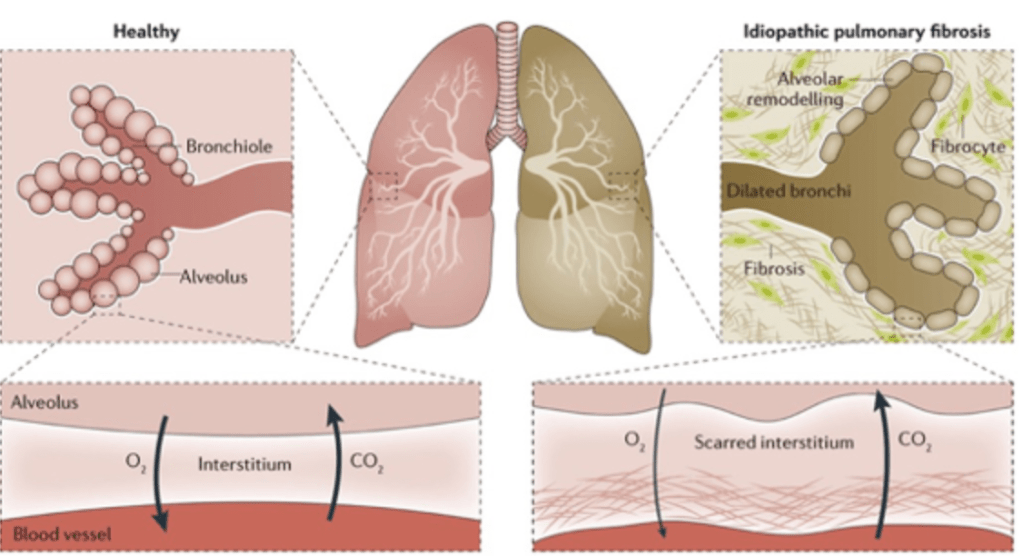
Question 56:
Answer: A) Sarcoidosis
Explanation:
The patient presents with symptoms including dyspnoea, non-productive cough, and fatigue, and has erythema nodosum and bilateral hilar lymphadenopathy on examination. Chest X-ray shows bilateral reticulonodular opacities, and CT reveals ground-glass opacities and fibrotic changes, especially in the upper lobes. Granulomas on biopsy are a key finding suggesting a granulomatous lung disease. Granulomas involve infiltration of immune cells such as macrophages due to the inability of destroying the pathogen. This causes inflammation. Sarcoidosis is the most likely diagnosis, as it is characterised by non-caseating granulomas and often presents with bilateral hilar lymphadenopathy, erythema nodosum, and upper-lobe involvement, even in the absence of specific antigen exposure.
Option B is incorrect because hypersensitivity pneumonitis (HP) is typically associated with a known exposure to organic antigens, such as bird droppings or mould. This patient does not have any reported exposure history to such antigens.
Option C is incorrect because non-specific interstitial pneumonia (NSIP) usually presents with more diffuse, subpleural fibrosis and does not typically show granulomas on biopsy.
Option D is incorrect because tuberculosis usually presents with a history of exposure to risk factors such as contact with infected individuals, recent travel, or immunosuppression. This patient does not have a clear history or findings typical of tuberculosis.
Option E is incorrect because idiopathic pulmonary fibrosis (IPF) typically presents with progressive dyspnoea, a dry cough, and basal fibrosis without granulomas. The upper-lobe involvement and granulomas in this case are more consistent with sarcoidosis.
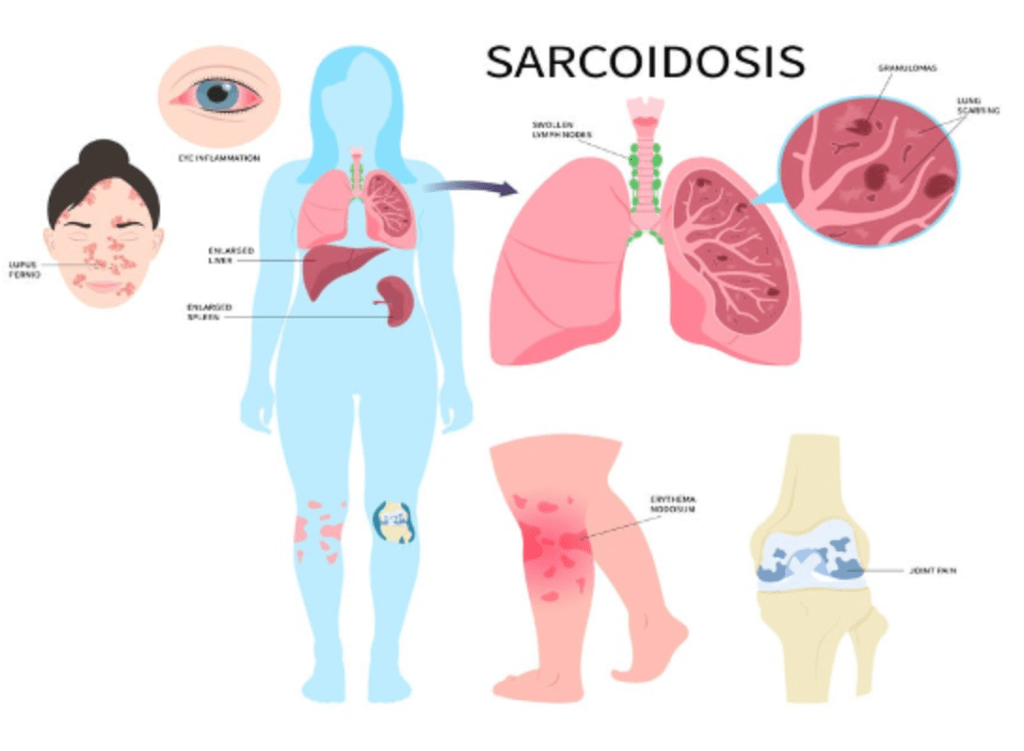
Question 57:
Answer: C) Increased insulin levels in the foetus
Explanation:
Increased insulin levels in the foetus, which can result from uncontrolled maternal diabetes, are known to inhibit surfactant production. High insulin levels act as an antagonist to cortisol, which is essential for surfactant synthesis. This results in delayed or decreased surfactant production, which can increase the risk of respiratory distress syndrome in the neonate.
Option A is incorrect because the administration of glucocorticoids is actually used to promote surfactant production in the preterm foetus, especially in the setting of preterm labour, by accelerating lung maturation.
Option B is incorrect because hypothermia during labour can cause a range of complications, including inactivation of surfactant but not decreasing its production. It is more associated with neonatal hypothermia and its associated risks.
Option D is incorrect because maternal beta-adrenergic drugs, used in preterm labour management, are more likely to reduce uterine contractions and delay labour. They do not decrease surfactant production, in fact they do the complete opposite.
Option E is incorrect because thyroid hormones are not known to directly impact surfactant production. While thyroid hormones affect many bodily functions, they are not involved in surfactant regulation.
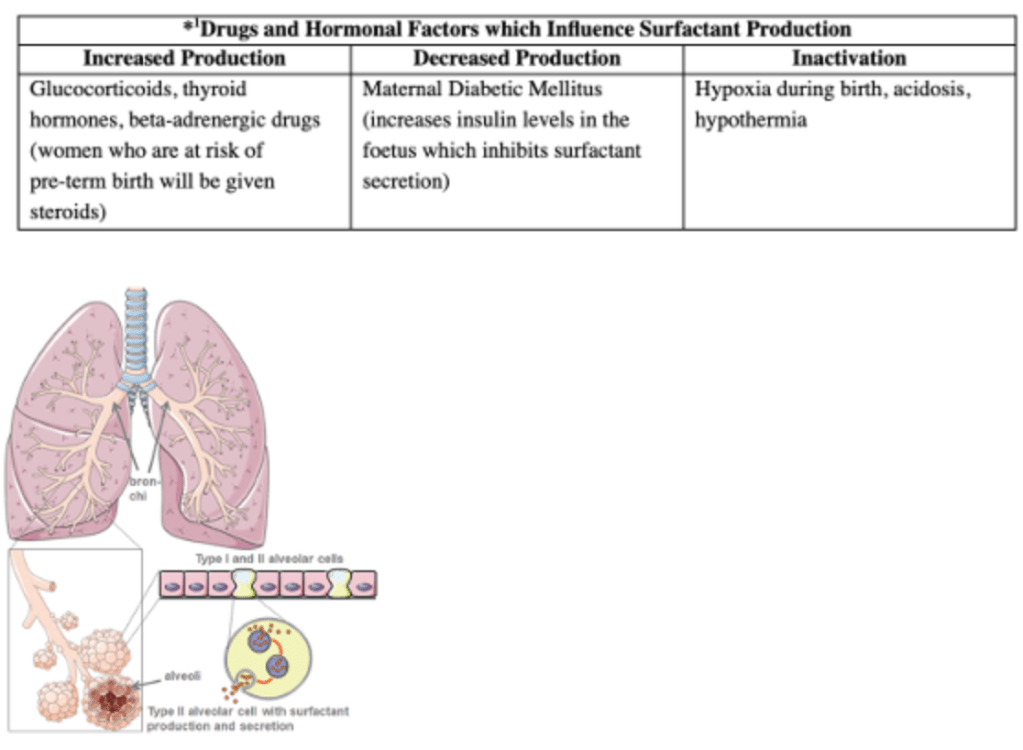
Question 58:
Answer: D) Reduced fetal glucocorticoid production
Explanation: Neonatal respiratory distress syndrome (RDS) is primarily caused by insufficient surfactant production in the lungs, which is critical for maintaining alveolar stability and preventing collapse after birth. The factors that promote surfactant production and lung maturation include the production of glucocorticoids. During labour, increased fetal glucocorticoid production promotes surfactant synthesis. In a caesarean section without prior labour, there is reduced stress and thus less glucocorticoid release, which can contribute to the development of RDS.
Option A is incorrect because increased catecholamine production during labour helps in lung maturation by stimulating surfactant production and promoting lung expansion after birth.
Option B is incorrect because increased thoracic squeeze during vaginal delivery helps to clear fluid from the lungs and contributes to the maturation of the respiratory system, reducing the risk of RDS.
Option C is incorrect because increased thyroid hormone release during labour also aids in the maturation of the lungs and the production of surfactant, reducing the risk of RDS.
Option E is incorrect because increased amniotic fluid clearance during labour helps to clear fluid from the lungs, which contributes to improved respiratory function and can reduce the severity of RDS.
Question 59:
Answer: B) Absence, hypoplasia, or dysplasia of bronchial cartilage
Explanation: Congenital lobar emphysema (CLE) is a condition where there is overinflation of one or more lobes of the lung, often due to an abnormality in the bronchial structure. The most common underlying cause of CLE is the absence, hypoplasia, or dysplasia of bronchial cartilage. This leads to airway collapse, resulting in air trapping and subsequent lung overdistention and emphysema. The collapsed lung seen on the X-ray is consistent with this pathology.
Option A is incorrect because increased bronchial cartilage thickness would typically cause airway narrowing rather than the overinflation seen in CLE.
Option C is incorrect because excessive surfactant production is more commonly associated with conditions like neonatal respiratory distress syndrome (NRDS), not CLE.
Option D is incorrect because pulmonary venous return anomalies typically cause symptoms related to heart failure and pulmonary oedema, not lobar emphysema.
Option E is incorrect because congenital diaphragmatic hernia is a separate congenital condition that results in abdominal contents herniating into the chest cavity and can lead to lung hypoplasia and respiratory distress, but it is not a cause of congenital lobar emphysema.
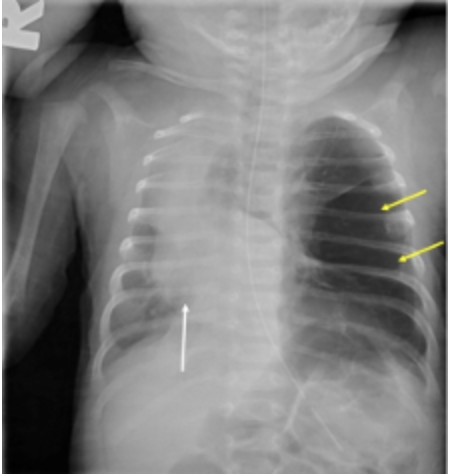
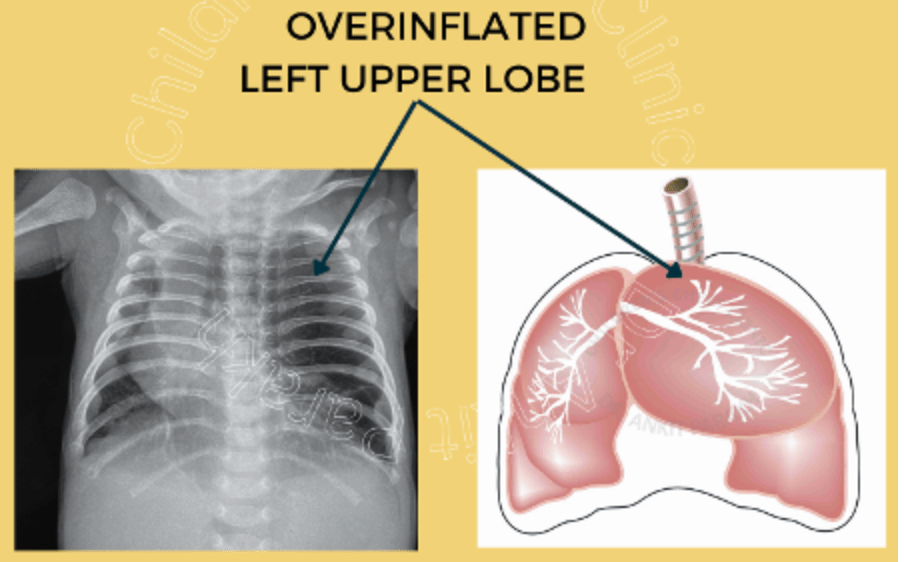
Question 60:
Answer: B) A patent ductus arteriosus causing deoxygenated blood flow
Explanation: Persistent pulmonary hypertension of the newborn (PPHN) is characterised by elevated pulmonary vascular resistance, leading to right-to-left shunting of blood through fetal circulatory structures, most notably the patent ductus arteriosus (PDA) and the foramen ovale. This results in the mixing of oxygenated and deoxygenated blood, causing cyanosis and respiratory distress. In PPHN, the PDA remains open, which allows deoxygenated blood from the right side of the heart to bypass the lungs and enter systemic circulation, leading to hypoxia.
Option A is incorrect because maternal polyhydramnios, although associated with some fetal conditions, does not directly cause persistent pulmonary hypertension.
Option C is incorrect because congenital cystic adenomatoid malformation (CCAM) involves a lung malformation that can lead to respiratory distress but does not typically cause persistent pulmonary hypertension directly.
Option D is incorrect because surfactant deficiency, which can occur in premature infants, leads to respiratory distress syndrome (RDS), not persistent pulmonary hypertension. PPHN may be seen in premature infants but is not caused by surfactant deficiency alone.
Option E is incorrect because while mechanical ventilation can contribute to lung injury (e.g., ventilator-associated lung injury or barotrauma), it is not the primary cause of persistent pulmonary hypertension. The underlying issue in PPHN is abnormal pulmonary vascular resistance, not mechanical ventilation.
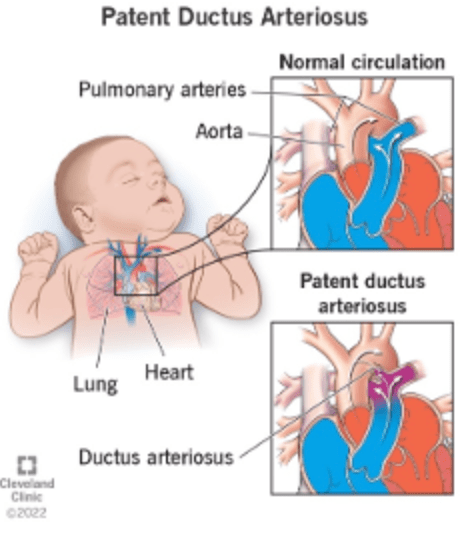
Question 61:
Answer: A) Maternal smoking during pregnancy leading to epigenetic changes
Explanation: The child presents with classic asthma symptoms, including recurrent wheezing, cough, and chest tightness, which are triggered by allergens like dust mites and pet dander. A family history of asthma and the presence of airway inflammation, indicated by the elevated fractional exhaled nitrous oxide (FeNO) level, further support the diagnosis. Maternal smoking during pregnancy is a well-established risk factor for the development of asthma in children. Smoking exposure in utero leads to epigenetic changes that can predispose the child to asthma, often through the promotion of airway inflammation and immune system alterations.
Option B is incorrect because while maternal smoking is a risk factor, a history of transient early wheeze, especially associated with maternal smoking, does not directly explain the development of persistent asthma in this child.
Option C is incorrect because a non-atopic wheeze typically arises from viral infections or other factors that do not involve an IgE-mediated allergic response. This child’s symptoms are more consistent with atopic asthma, which is triggered by allergens such as dust mites & pet dander.
Option D is incorrect because the child’s symptoms, including the elevated FeNO level (>35ppb), suggest an IgE-mediated allergic response to environmental allergens. The presence of day-to-day variability in peak flow readings further supports this.
Option E is incorrect because elevated FeNO levels (>35ppb) and airway inflammation suggest active eosinophilic inflammation, which is a hallmark of asthma, rather than a lack of eosinophil activity.
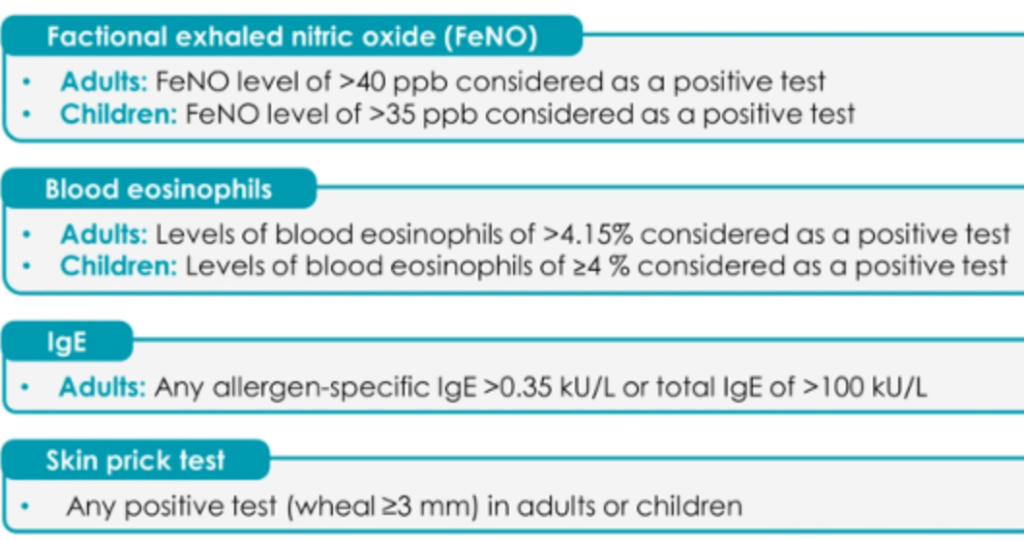
Question 62:
Answer: B) Enhanced B-cell production of IgE in response to IL-4 and IL-13, promoting mast cell degranulation
Explanation: This child presents with classic signs of asthma, including recurrent wheezing, cough, and exacerbations triggered by pollen exposure. Spirometry shows reversible airflow obstruction, and the presence of eosinophils in sputum, along with elevated fractional exhaled nitric oxide (FeNO) levels, indicates ongoing Type 2 inflammation, characteristic of allergic asthma. The immunopathology of asthma involves the activation of T-helper 2 (TH2) cells, which release interleukins such as IL-4 and IL-13. These interleukins promote B-cell differentiation and increased production of IgE. The IgE binds to mast cells, leading to their degranulation and the release of inflammatory mediators, contributing to the asthma symptoms. TH2 also stimulates the release of IL-5 which activates eosinophils.
Option A is incorrect because TH17 cells are involved in neutrophilic inflammation and conditions like chronic obstructive pulmonary disease (COPD) or certain autoimmune diseases, but not in the typical pathogenesis of allergic asthma.
Option C is incorrect because TH1-mediated responses are typically associated with conditions like tuberculosis and other infections, not allergic asthma. Asthma is more commonly driven by TH2 responses.
Option D is incorrect because while leukotrienes are important mediators in asthma, the primary mechanism for this child’s asthma is the TH2-driven IgE production and mast cell degranulation, not an overproduction of leukotrienes alone.
Option E is incorrect because asthma primarily involves bronchoconstriction and airway inflammation rather than a loss of airway smooth muscle contractility. Chronic inflammation and remodelling can lead to airway narrowing and fibrosis over time, but loss of smooth muscle contractility is not a primary feature.
Question 63:
Answer: E) Bronchodilator reversibility test improvement of >12%/200 mL
Explanation:
The most diagnostic test for asthma in this patient is the bronchodilator reversibility test, which shows an improvement in FEV1 by more than 12% and at least 200 mL following administration of a bronchodilator such as salbutamol. This confirms reversible airway obstruction, a hallmark of asthma.
Option A is incorrect because although an FEV1/FVC ratio <70% is consistent with obstructive airway disease, it is not specific for asthma and could also indicate other conditions such as COPD.
Option B is incorrect because peak flow variability of >20% supports the diagnosis of asthma but is less specific than the bronchodilator reversibility test.
Option C is incorrect because a positive skin prick test indicates atopy and allergen sensitivity, which are common in asthma but do not confirm the diagnosis.
Option D is incorrect because a FeNO level of 45 ppb suggests eosinophilic airway inflammation, which is supportive of asthma but not definitive on its own.
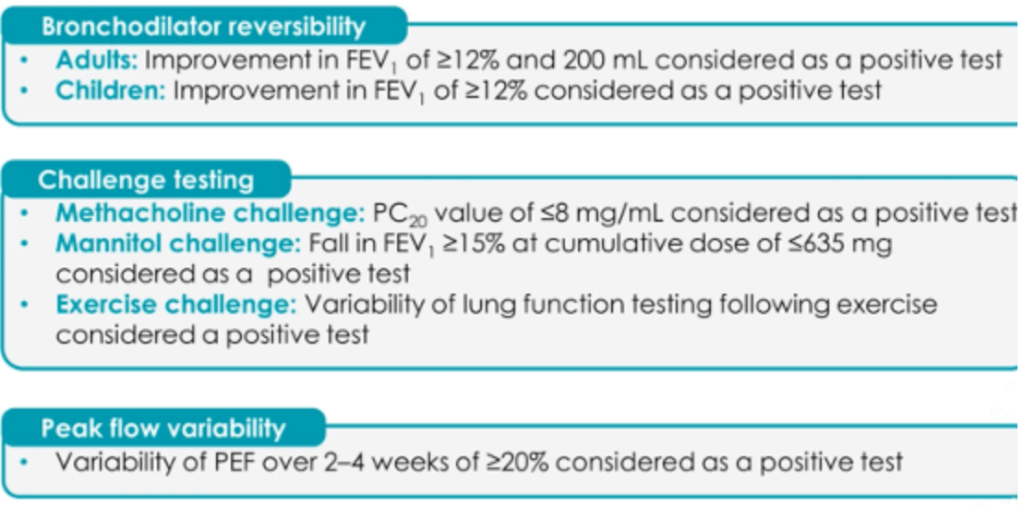
Question 64:
Answer: C) Mixed Sleep Apnoea
Explanation:
Mixed sleep apnoea is characterised by the coexistence of features of both obstructive sleep apnoea (OSA) and central sleep apnoea (CSA). This patient’s polysomnography findings show periods of cessation of airflow with continued respiratory effort (consistent with OSA) and periods of complete cessation of airflow with no respiratory effort (consistent with CSA). The combination of these findings makes mixed sleep apnoea the most likely diagnosis.
Option A is incorrect because central sleep apnoea involves cessation of breathing due to a lack of respiratory effort, but it does not explain the periods of airflow cessation with continued effort seen in this case.
Option B is incorrect because obstructive sleep apnoea typically involves airway obstruction with continued respiratory effort but does not include periods of absent respiratory effort.
Option D is incorrect because Cheyne-Stokes breathing is characterised by a cyclical pattern of waxing and waning respiratory effort with central apnoea, commonly seen in heart failure, but it does not include obstructive apnoea.
Option E is incorrect because the polysomnography findings are not specific for drug-induced CSA, and the patient’s history does not indicate a cause such as opioid use.
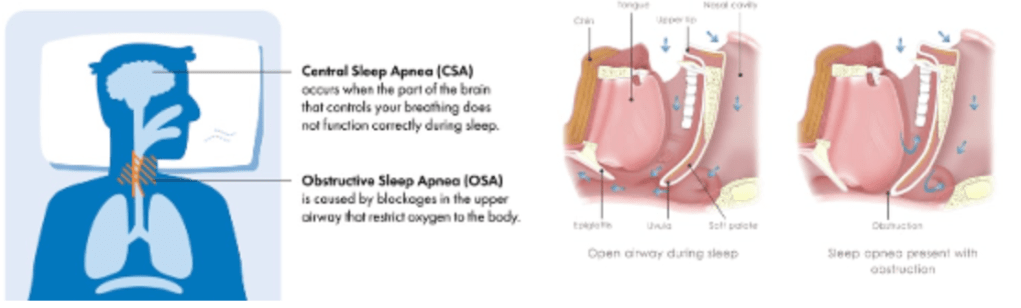
Question 65:
Answer: A) Loss of orexin-producing neurons in the lateral hypothalamus
Explanation:
The patient presents with excessive daytime sleepiness, cataplexy (sudden loss of muscle tone triggered by emotions), sleep paralysis, and vivid hypnagogic hallucinations, all of which are characteristic of narcolepsy type 1. This condition is caused by the loss of orexin (hypocretin)-producing neurons in the lateral hypothalamus, leading to dysregulation of sleep-wake cycles.
Option B is incorrect because dysfunction of the brainstem responsible for respiratory control is associated with central sleep apnoea, not narcolepsy.
Option C is incorrect because overactivation of the sympathetic nervous system might lead to conditions such as insomnia or anxiety but does not account for the symptoms seen here.
Option D is incorrect because insufficient dopamine production in the substantia nigra is associated with Parkinson’s disease, which presents with motor symptoms like tremors and rigidity, not the features described in this case.
Option E is incorrect because genetic mutations affecting circadian rhythm regulation, such as those in familial advanced sleep phase syndrome, would primarily cause shifts in sleep timing, not the classic features of narcolepsy like cataplexy and sleep paralysis.
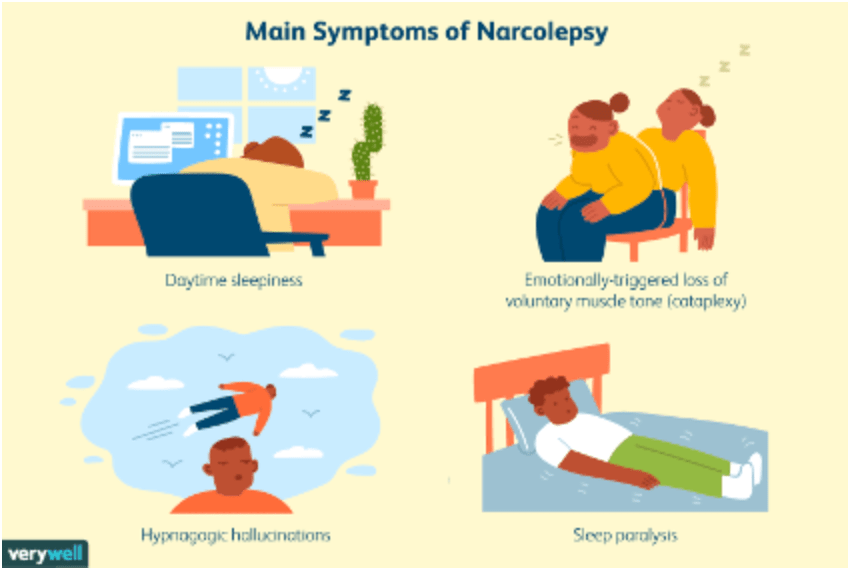
Question 66:
Answer: C) REM Sleep Behaviour Disorder
Explanation:
The patient’s symptoms, including acting out dreams during the latter part of the night and unawareness of the events upon waking, are characteristic of REM Sleep Behaviour Disorder (RBD). This condition involves the loss of normal muscle atonia during REM sleep, allowing the person to physically act out their dreams. RBD is often associated with neurodegenerative disorders like Parkinson’s disease.
Option A is incorrect because Restless Leg Syndrome typically presents with an urge to move the legs, often accompanied by uncomfortable sensations, and is unrelated to acting out dreams. It is often due to an iron deficiency affecting GABA production or due to medications.
Option B is incorrect because Non-REM Parasomnias, such as sleep walking or talking, occur during non-REM sleep (earlier in the night).
Option D is incorrect because narcolepsy is characterised by excessive daytime sleepiness, cataplexy, and other features such as sleep paralysis and vivid hypnagogic hallucinations, not violent behaviour during sleep.
Option E is incorrect because sleepwalking (somnambulism) occurs during non-REM sleep and typically does not involve vivid dream enactment or association with Parkinson’s disease.
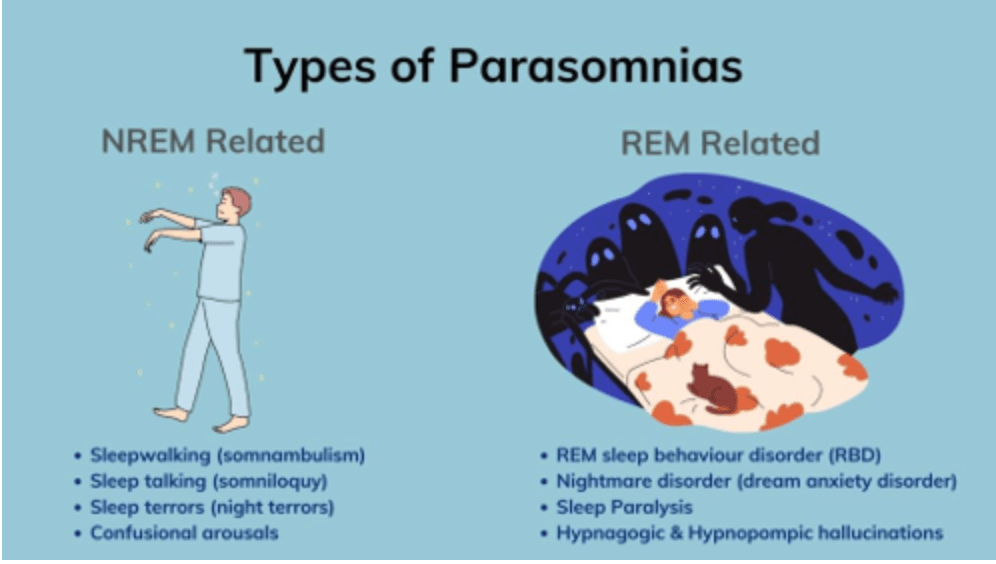
Question 67:
Answer: A) Inactivation of α1-antitrypsin leading to unchecked elastin breakdown
Explanation:
The patient’s symptoms, long smoking history, and pulmonary function test findings are consistent with chronic obstructive pulmonary disease (COPD), specifically emphysema. In emphysema, smoking causes oxidative stress and inflammation, leading to the inactivation of α1-antitrypsin. This allows unchecked elastase activity, resulting in the breakdown of elastin in the alveolar walls and loss of elastic recoil, contributing to airflow obstruction and hyperinflation.
Option B is incorrect because surfactant deficiency is more relevant in neonatal respiratory distress syndrome and not in COPD.
Option C is incorrect because increased mucus production is characteristic of chronic bronchitis, another form of COPD, but it does not explain the primary mechanism in emphysema.
Option D is incorrect because excessive IgE production and bronchial hyperresponsiveness are hallmark features of asthma, not COPD.
Option E is incorrect because increased capillary permeability causing pulmonary oedema is a feature of conditions like acute respiratory distress syndrome (ARDS) or left-sided heart failure, not COPD.
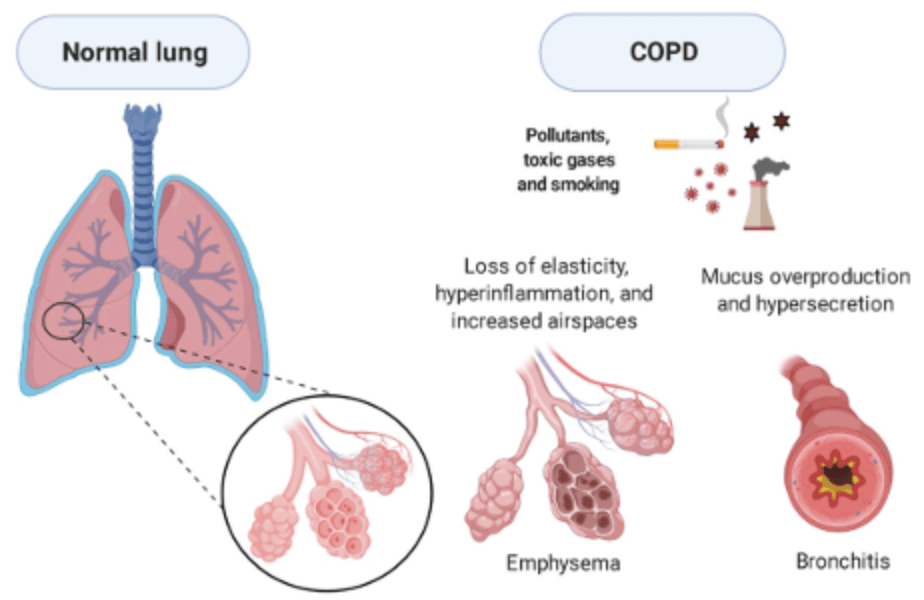
Question 68:
Answer: C) Extra-pleural pathology
Explanation:
The radiological findings of an irregular mass in the lower left hemithorax with evidence of rib destruction suggest an extra-pleural origin. Extra-pleural masses, such as metastatic deposits, mesothelioma, or soft tissue tumours, can cause rib destruction and have irregular borders due to their invasive nature (INCOMPLETE BORDER SIGN!!!). These features help distinguish extra-pleural masses from intra-pulmonary or pleural pathologies.
Option A is incorrect because pulmonary pathologies, such as lung tumours or infections, typically do not cause rib destruction and would have a different radiological appearance (COMPLETE BORDER SIGN!!!).
Option B is incorrect because pleural pathologies like pleural effusions or plaques rarely lead to rib destruction and would usually present with other characteristic features such as fluid accumulation (INCOMPLETE BORDER SIGN WITH NO RIB DESTRUCTION).
Option D is incorrect because benign lung nodules, such as granulomas or hamartomas, typically have well-defined, smooth borders and do not invade surrounding structures like ribs.
Option E is incorrect because pneumonia is an infectious process that presents with consolidation and air bronchograms, not a mass with rib destruction.
D-C = complete border sign suggestive of a pulmonary lesion/tumour.
A-B = Incomplete border sign (curved edge which is then diffused) with RIB DESTRUCTION indicative of an extrapleural pathology.
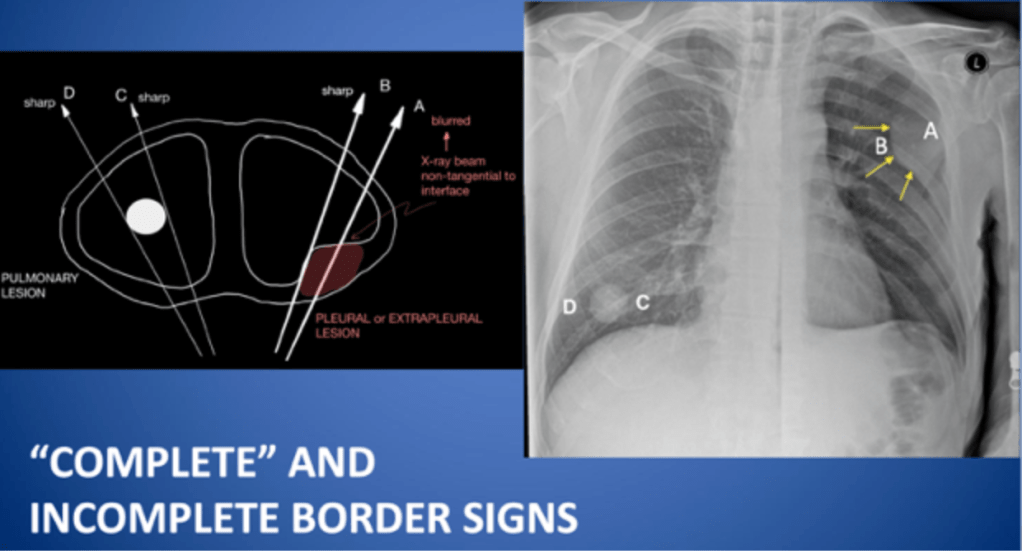
Question 69:
Correct Answer: A. Posterior cricoarytenoid
- The posterior cricoarytenoid muscle is the only muscle responsible for abducting the vocal cords.It moves the arytenoid cartilages outward, opening the glottis and allowing airflow during inspiration. This is a critical function for maintaining an open airway
Explanation of Each Answer Option.
B. Lateral cricoarytenoid
- Incorrect: This muscle adducts the vocal cords, bringing them together to close the glottis during phonation.
- It works opposite to the posterior cricoarytenoid.
C. Thyroarytenoid
- Incorrect: The thyroarytenoid shortens and relaxes the vocal cords, which lowers the pitch of the voice.
- It does not contribute to opening the glottis.
D. Cricothyroid
- Incorrect: The cricothyroid muscle lengthens and tenses the vocal cords by tilting the thyroid cartilage forward, raising the pitch of the voice.
- It is unrelated to the abduction of the vocal cords.
E. Interarytenoid
- Incorrect: The interarytenoid muscle adducts the vocal cords by bringing the arytenoid cartilages together, assisting in glottic closure during phonation or swallowing.
- It does not assist in abduction.
Question 70:
Correct Answer: A. Parainfluenza virus
- The parainfluenza virus (especially types 1 and 2) is the most common cause of croup, accounting for the majority of cases. It causes inflammation and narrowing of the subglottic region, leading to the characteristic barking cough and stridor. Typical treatment is dexamethasone.
Explanation of Each Answer Option.
B. Respiratory syncytial virus (RSV)
- Incorrect: While RSV is a major cause of bronchiolitis and lower respiratory tract infections in children, it is not the primary cause of croup.
C. Influenza virus
- Incorrect: Influenza can rarely cause croup but more commonly presents with fever, myalgia, and respiratory symptoms. It is not a leading cause of croup.
D. Adenovirus
- Incorrect: Adenovirus is associated with upper respiratory tract infections and pharyngoconjunctival fever but is a rare cause of croup.
E. Streptococcus pyogenes
- Incorrect: This bacterium is a cause of bacterial infections such as strep throat and tonsillitis, not viral croup. However, bacterial superinfection (bacterial tracheitis) can sometimes complicate croup.
Question 71:
Correct answer: E
Based on the patient’s presentation it makes most sense to be empyema- a collection of pus in the pleural cavity. Furthermore in the CXR we can see in the right lower lobe it is covered, therefore suggesting empyema.
Incorrect answer options
- Pleural effusion: Incorrect, whilst based on the CXR alone it would be reasonable to assume ti is a pleural effusion however based on the symptoms of the patient having fever it indicated towards an infection and hence Empyema is more correct.
- Pneumonia: incorrect, based on the symptoms it would be fair to choose pneumonia however based on the CXR we can clearly see an empyema on the RHS therefore E is the right answer option.
- Emphysema: incorrect, Emphysema which is a condition where the walls of the alveoli sac breakdown and fuse together reducing the surface area to volume ratio. However based on the symptoms it is not suggestive of this condition as you do not tend to get fever/ pyrexia from this condition.
- ILD incorrect, this is due to the fact that there is a productive cough which is typically the opposite in ILD as ILD produced a dry cough furthermore no indication of ILD on CXR.
Question 72:
Correct Answer: A. Surfactant deficiency
- Correct: Surfactant deficiency is the hallmark of respiratory distress syndrome (RDS) in preterm neonates.
- Surfactant reduces alveolar surface tension; its deficiency leads to alveolar collapse, impaired gas exchange, and respiratory distress.
- This condition is common in neonates born before 32 weeks due to immature type II pneumocytes, which produce surfactant.
Explanation of Each Answer Option
B. Persistent pulmonary hypertension of the newborn (PPHN)
- Incorrect: PPHN occurs due to the failure of normal circulatory transition at birth, resulting in persistent right-to-left shunting and hypoxemia.
- It typically presents with severe cyanosis, but the chest X-ray is often normal or shows mild cardiomegaly, unlike the ground-glass appearance seen in RDS.
C. Transient tachypnea of the newborn (TTN)
- Incorrect: TTN results from delayed clearance of fetal lung fluid and is more common in term or near-term infants.
- Chest X-ray findings in TTN include hyperinflation with fluid in the fissures, not the ground-glass appearance seen in RDS.
D. Meconium aspiration syndrome (MAS)
- Incorrect: MAS occurs when a neonate inhales meconium-stained amniotic fluid, leading to airway obstruction, inflammation, and chemical pneumonitis.
- It is seen in term or post-term infants with a history of meconium-stained amniotic fluid, and the chest X-ray shows patchy opacities rather than a diffuse ground-glass appearance.
E. Congenital diaphragmatic hernia (CDH)
- Incorrect: CDH is caused by herniation of abdominal contents into the thoracic cavity, impairing lung development.
- It presents with scaphoid abdomen, respiratory distress, and chest X-ray findings showing bowel loops in the thorax, which are distinct from RDS.
Question 73:
Correct Answer: D Chronic obstructive pulmonary disease (COPD)
- Correct: The reduced FEV1/FVC ratio (<70%) is indicative of an obstructive lung disease.
- FEV1 <80% of predicted shows moderate airflow limitation, consistent with COPD.
- The decreased DLCO suggests emphysema, a common component of COPD, due to alveolar destruction.
Explanation of Each Answer Option
A. Neuromuscular disorder
- Incorrect: Neuromuscular disorders cause a restrictive pattern, with reduced FVC and TLC but a normal or elevated FEV1/FVC ratio (>0.7)
- DLCO is generally normal unless there is associated parenchymal lung disease or reduced effort affecting the test.
B. Idiopathic pulmonary fibrosis (IPF)
- Incorrect: IPF is a restrictive lung disease, characterized by a normal or elevated FEV1/FVC ratio with reduced FVC and total lung capacity (TLC).
- DLCO is also reduced, but the pattern in this case (reduced FEV1/FVC ratio) does not fit a restrictive disease.
C. Asthma
- Incorrect: Asthma is an obstructive lung disease, but it is usually reversible with bronchodilator therapy.
- In asthma, DLCO is typically normal or elevated, unlike the reduced DLCO seen in this case, which points to structural lung damage (e.g., emphysema).
E. Pulmonary embolism (PE)
- Incorrect: PE may cause an isolated reduction in DLCO due to impaired perfusion in the pulmonary capillary bed.
- However, spirometry (FEV1, FVC, FEV1/FVC ratio) is usually normal in PE, unlike the obstructive pattern seen in this case.
Question 74:
Correct Answer: B. Spirometry with bronchodilator reversibility testing
- Correct: Spirometry is the gold standard for diagnosing asthma in children over 5 years old.
- Findings in asthma: Reduced FEV1/FVC ratio that improves significantly (>12% increase in FEV1) after bronchodilator therapy, confirming reversible airway obstruction.
Explanation of Each Answer Option
A. Chest X-ray to rule out structural abnormalities
- Incorrect: A chest X-ray may be helpful to exclude structural or other causes of respiratory symptoms, such as foreign body aspiration or pneumonia, but it does not diagnose asthma.
C. Skin prick testing for aeroallergens
- Incorrect: Skin prick testing identifies atopy and sensitivities to specific allergens, which are risk factors for asthma. However, it does not confirm the diagnosis of asthma itself.
D. Serum IgE and eosinophil count
- Incorrect: Elevated IgE and eosinophil levels indicate allergic inflammation and may support the diagnosis of atopy or allergic asthma. However, these findings are not diagnostic for asthma.
E. Peak expiratory flow monitoring over several weeks
- Incorrect: Peak expiratory flow (PEF) monitoring can help assess variability in airway obstruction over time, supporting an asthma diagnosis. However, it is less sensitive and specific than spirometry, particularly in young children.
Question 75:
Correct Answer: A. Add a long-acting beta-agonist (LABA) to her ICS
- Adding a LABA to ICS is the next step for managing asthma that is not well-controlled with medium-dose ICS alone.
- LABA/ICS combinations provide better symptom control and reduce exacerbations compared to increasing ICS dose alone.
Explanation of Each Answer Option
B. Switch to a leukotriene receptor antagonist (LTRA) as monotherapy
- Incorrect: LTRAs (e.g., montelukast) can be considered as add-on therapy, especially for patients with allergic rhinitis or exercise-induced asthma.
- However, monotherapy with LTRA is less effective than ICS/LABA combinations for persistent asthma.
C. Increase her ICS dose to high-dose therapy
- Incorrect: While increasing the ICS dose is an option, it is less effective than adding a LABA. High-dose ICS alone increases the risk of side effects without significantly improving outcomes compared to combination therapy.
D. Add a long-acting muscarinic antagonist (LAMA)
- Incorrect: LAMAs (e.g., tiotropium) are used as add-on therapy for patients who remain uncontrolled on ICS/LABA therapy or have features of asthma-COPD overlap.
- This step is premature without first adding a LABA to ICS.
E. Refer for biologic therapy targeting interleukin-5 (IL-5)
- Incorrect: IL-5 inhibitors (e.g., mepolizumab) are reserved for severe eosinophilic asthma that remains uncontrolled despite high-dose ICS/LABA therapy and other add-ons.
- This patient does not yet meet the criteria for biologic therapy.
Question 76:
Correct Answer: C. The presence of excessive daytime sleepiness
- Correct: Excessive daytime sleepiness is what differentiates OSA syndrome (OSAS) from asymptomatic OSA.
- OSA involves apneas/hypopneas without necessarily causing significant symptoms, while OSAS includes daytime functional impairment, such as sleepiness.
Explanation of Each Answer Option
A. The presence of an elevated AHI
- Incorrect: An elevated AHI (≥5 events/hour) is diagnostic of OSA but does not distinguish OSA from OSAS.
- OSA refers to the physiological events (apneas and hypopneas), regardless of symptoms.
B. The presence of obesity as a risk factor
- Incorrect: Obesity is a common risk factor for both OSA and OSAS but does not define the syndrome.
D. The occurrence of loud snoring and witnessed apneas
- Incorrect: Snoring and witnessed apneas occur in both OSA and OSAS and do not differentiate the two conditions.
E. The association with an increased risk of cardiovascular disease
- Incorrect: Both OSA and OSAS are associated with an increased risk of cardiovascular disease, including hypertension, atrial fibrillation, and stroke.
Question 77:
Correct Answer: B. T10
- Correct: The oesophageal hiatus, which transmits the oesophagus (10 letters hence T10), the vagus nerves, and small esophageal blood vessels, is located at the T10 vertebral level.
- Pathologies such as hiatal hernias involve this opening.
Explanation of Each Answer Option
A. T8
- Incorrect: The T8 level corresponds to the caval opening in the diaphragm, which allows the inferior vena cava (vena cava has 8 letters hence T8) (IVC) and branches of the right phrenic nerve to pass through.
C. T4
- Incorrect: this is above the diaphragm and where the trachea bifurcates into the primary bronchi.
D. T11
- Incorrect: The T11 level is below the diaphragm and does not correspond to a major opening in the diaphragm.
E. T12
- Incorrect: The aortic hiatus which transmits the aorta, cisterna chyli ( (12 letters hence t12), and sometimes the azygos vein, is located at the T12 level.
Question 78:
Correct Answer: D. Poor reversibility of airflow obstruction
- Correct: COPD is characterized by poor or absent reversibility of airflow obstruction following bronchodilator therapy, while asthma typically shows significant reversibility (FEV1 improvement ≥12% and 200 mL).in this patient, the minimal improvement in FEV1 strongly suggests COPD rather than asthma.
Explanation of Each Answer Option
A. A reduced FEV1/FVC ratio on spirometry
- Incorrect: A reduced FEV1/FVC ratio (<70%) is a feature of both COPD and asthma and does not differentiate between the two.
B. History of smoking
- Incorrect: Smoking is a significant risk factor for COPD but does not exclude asthma. Some asthma patients may also smoke or have a smoking history.
C. Presence of wheezing and dyspnea
- Incorrect: Both COPD and asthma commonly present with wheezing and dyspnea. These symptoms alone cannot distinguish between the two conditions.
E. Onset of symptoms in adulthood
- Incorrect: While COPD often begins in adulthood, adult-onset asthma is also possible. Onset age alone does not reliably distinguish between the two conditions.
Question 79:
Correct Answer: E. Alpha-1 antitrypsin deficiency
- Correct: Alpha-1 antitrypsin deficiency is a rare inherited condition that predisposes patients to early-onset COPD, particularly basal panacinar emphysema, even in non-smokers. It results from a deficiency of alpha-1 antitrypsin, which protects lung tissue from proteolytic enzymes like elastase.
Explanation of Each Answer Option
A. Cystic fibrosis
- Incorrect: Cystic fibrosis primarily affects the lungs due to thickened mucus and recurrent infections but is not typically associated with COPD in non-smokers.it is more commonly diagnosed in childhood and involves additional systemic features.
B. connective tissue disorder
- Incorrect: connective tissue disorder may cause lung complications, such as pneumothorax, but it does not cause COPD or emphysema.
C. Kartagener syndrome
- Incorrect: Kartagener syndrome is a subset of primary ciliary dyskinesia characterized by recurrent respiratory infections, sinusitis, and situs inversus. It does not typically result in COPD or emphysema.
D. Ehlers-Danlos syndrome
- Incorrect: Ehlers-Danlos syndrome, another connective tissue disorder, can cause lung complications like pneumothorax but does not cause emphysema or COPD.
Question: 80:
Correct answer: A
Option A (Correct Answer): The Wells score is a clinical tool used to assess the probability of a pulmonary embolism. If a patient’s score suggests a high clinical probability (typically ≥ 4), the next step is to proceed with imaging studies such as a CT pulmonary angiogram (CTPA), which is the gold standard for diagnosing PE. Therefore in this patient she would score at least 4.5 ( 3 for the swollen legs and 1.5 for the high HR) therefore the next best suitable option is to offer an immediate CTPA.

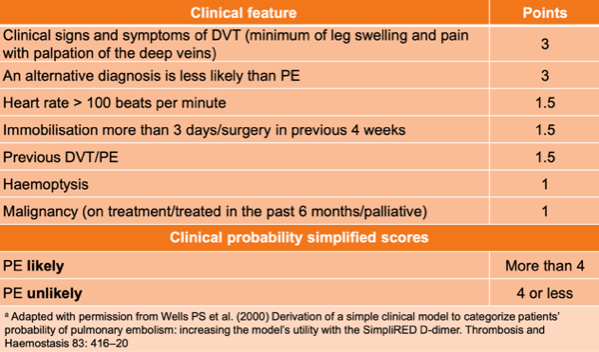
Explanation:
- Option B: A D-dimer test is typically used in low-risk patients (Wells score < 4) to rule out PE, but in high-probability cases, immediate imaging is recommended.
- Option C: While anticoagulation therapy (such as low-molecular-weight heparin) is indicated if PE is confirmed, it should not be given empirically without diagnostic confirmation.
- Option D: Observation and oxygen therapy are supportive measures but do not replace the need for a proper diagnosis of PE.
- Option E: A chest X-ray is useful in excluding other conditions, but it is not sufficient to diagnose PE, which requires more specific imaging such as CTPA.
Question 81:
Correct answer: A
- The S1Q3T3 pattern is classically associated with acute pulmonary embolism. This pattern consists of a deep S wave in lead I, a Q wave in lead III, and an inverted T wave in lead III. It suggests right heart strain due to increased pressure in the pulmonary arteries from a PE. You may also see sinus tachycardia (the heart rate is faster than normal due to the sinus node sending out electrical signals more quickly). You could also find on a PE patient a right bundle branch blocks on an ECG.
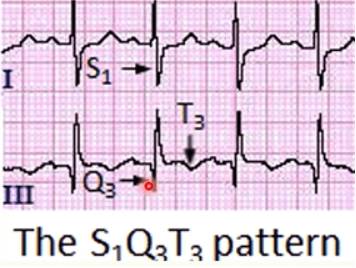
Explanation:
- Option A (Correct Answer): The S1Q3T3 pattern is classically associated with acute pulmonary embolism. This pattern consists of a deep S wave in lead I, a Q wave in lead III, and an inverted T wave in lead III. It suggests right heart strain due to increased pressure in the pulmonary arteries from a PE.
- Option B: A prolonged PR interval is typically associated with heart block and is not a characteristic finding in pulmonary embolism.
- Option C: Left axis deviation can be seen in a variety of conditions, including left ventricular hypertrophy or conduction abnormalities, but it is not typically associated with PE.
- Option D: Nonspecific ST-segment and T-wave changes (such as ST depression or T-wave inversion) can be seen in a wide variety of conditions, including PE, but they are not as specific or characteristic as the S1Q3T3 pattern.
- Option E: Ventricular tachycardia is a serious arrhythmia but is not a common or expected finding in pulmonary embolism. PE typically causes right ventricular strain, which leads to other ECG findings.
Question 82:
Correct answer: D
Adenocarcinoma is the most common subtype of non-small cell lung cancer (NSCLC) in patients who are non-smokers and is strongly associated with EGFR mutations. Targeted therapy against EGFR mutations (e.g., erlotinib, gefitinib) has been shown to be effective in treating EGFR-mutated adenocarcinoma.EGFR mutations can be treated with TKI’s– tyrosine kinase inhibitors, are a type of targeted therapy and cancer growth blocker drug
Explanation:
- Option A: Small cell lung cancer (SCLC) is a highly aggressive cancer associated with smoking, and it is not typically associated with EGFR mutations.
- Option B: Squamous cell carcinoma is also a type of NSCLC but is more commonly associated with smoking and is not typically linked to EGFR mutations.
- Option C: Large cell carcinoma is a subtype of NSCLC, but it is not specifically linked to EGFR mutations and is more poorly differentiated than adenocarcinoma.
- Option E: Carcinoid tumors are a rare type of lung cancer that are typically well-differentiated and not associated with EGFR mutations.
Question:83:
Correct answer: A
Squamous cell carcinoma is a subtype of non-small cell lung cancer (NSCLC) commonly associated with smoking and often presents with hypercalcemia due to the secretion of parathyroid hormone-related protein (PTHrP). Parathyroid hormone-related protein (PTHrP) is a protein that is often expressed in lung cancer and can play a role in the progression of the disease. This condition can cause hypercalcemia, which is a classic feature of squamous cell carcinoma.
Explanation:
- Option B: Small cell lung cancer (SCLC) is a highly aggressive cancer often associated with smoking but typically does not present with hypercalcemia. SCLC is more likely to cause symptoms related to paraneoplastic syndromes such as lambert Eaton syndrome, SIADH (syndrome of inappropriate antidiuretic hormone secretion= hyponatremia) and Cushing’s syndrome.
- Option C: Non-small cell lung cancer (adenocarcinoma) is the most common lung cancer in non-smokers and is not typically associated with hypercalcemia. It also tends to present in the peripheral lung tissue rather than centrally, as is seen in squamous cell carcinoma.
- Option D: Large cell carcinoma is another subtype of NSCLC but is not as commonly associated with hypercalcemia as squamous cell carcinoma.
- Option E: Pulmonary metastasis from another primary site is a possibility but is less likely given the patient’s history of heavy smoking and the presence of hypercalcemia, which is more characteristic of squamous cell carcinoma of the lung.
Question 84:
Correct answer: A
Type 2 Respiratory Failure due to chronic alveolar hypoventilation in ILD. In advanced ILD, progressive lung fibrosis and reduced compliance impair ventilation, leading to hypercapnia and hypoxemia, as seen in this ABG. Chronic compensation is reflected by elevated bicarbonate levels. T2RF is due to issues with ventilation therefore you would expect to see hypercapnia and hypoxia.
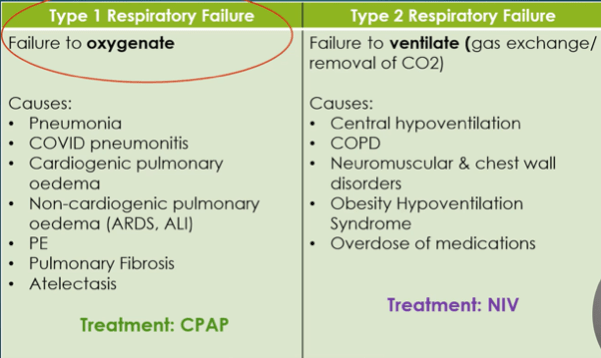
Explanation:
- Option B: Type 1 Respiratory Failure due to pulmonary fibrosis exacerbation. ILD often presents with T1RF due to impaired oxygen diffusion, but this patient’s elevated PaCO2 and acid-base status indicate hypoventilation consistent with T2RF.
- Option C: Metabolic acidosis with compensatory respiratory acidosis. This is incorrect because respiratory acidosis does not compensate for metabolic acidosis. The primary issue here is respiratory in origin, not metabolic.
- Option D: Mixed acid-base disorder with hypoxemia due to underlying lung disease. While mixed disorders can occur, the ABG findings (high PaCO2, low pH, high HCO3-) are more consistent with chronic respiratory acidosis due to T2RF without evidence of a metabolic disturbance.
- Option E: Type 2 Respiratory Failure due to advanced neuromuscular fatigue exacerbating ILD. Neuromuscular fatigue can contribute to hypoventilation in chronic lung diseases, but there is no clinical indication in this case (e.g., significant muscular weakness or prior neuromuscular disease) to support this explanation. The underlying issue remains primarily respiratory due to ILD itself.
Question 85:
Correct answer: B
Elevated FeNO (50 ppb) and PEF variability (25%). Elevated FeNO indicates eosinophilic airway inflammation, strongly suggestive of asthma. PEF variability of ≥20% supports variable airway obstruction, another hallmark of asthma.
Explanation:
- Option A: l FEV1/FVC ratio (0.80) and non-reversible spirometry. An increased FEV1/FVC ratio would not be seen in asthma, this is due to the fact asthma is obstructive and causes a decrease in FEV1 therefore would cause a ratio to be <0.7.
- Option C: Non-reversible spirometry and normal FeNO after treatment (10 ppb). A normal FeNO after treatment suggests response to therapy but does not rule out asthma, especially with other supporting findings like elevated initial FeNO and PEF variability.
- Option D: Normal FeNO (10 ppb) and lack of bronchodilator reversibility. A single normal FeNO after treatment does not confirm or exclude asthma, particularly in the presence of other abnormal findings.
- Option E: Symptoms alone without supporting diagnostic findings. While asthma symptoms are important, the elevated FeNO and PEF variability provide strong objective evidence, making symptoms alone an insufficient basis for diagnosis in this case.
Question 86:
Correct answer C
Pulmonary hemorrhage is associated with an elevated DLCO/TLCO due to the increased availability of hemoglobin in the alveoli, which binds carbon monoxide, thereby falsely elevating the measurement.
Explanation:
- Option A: Chronic obstructive pulmonary disease (COPD) typically causes a decreased DLCO/TLCO due to destruction of alveolar-capillary units in emphysema.
- Option B: Pulmonary hypertension can reduce DLCO/TLCO because of impaired blood flow through the pulmonary capillaries. It does not typically elevate the value.
- Option D: Idiopathic pulmonary fibrosis (IPF) causes a reduced DLCO/TLCO due to thickened alveolar walls that impair gas exchange.
- Option E: Pneumothorax would result in a reduced DLCO/TLCO because of the loss of functional alveolar surface area for gas exchange.
Question 87:
Correct answer: B
2nd intercostal space, midclavicular line is the recommended site for needle decompression in tension pneumothorax. This site provides easy access to the pleural cavity with minimal risk to surrounding structures.
Explanation:
- Option A: 4th intercostal space, midaxillary line is a site often used for chest tube insertion, not for needle decompression.
- Option C: 5th intercostal space, anterior axillary line is another common site for chest tube placement, particularly for managing simple pneumothorax or pleural effusion, but not tension pneumothorax.
- Option D: 6th intercostal space, midscapular line is not used for pneumothorax management due to its posterior location and increased risk of complications.
- Option E: 3rd intercostal space, midclavicular line is not the standard recommendation for needle decompression, as the 2nd intercostal space is more accessible and widely used.
Question 88:
Correct answer A
Class I: Defective protein production. Class I mutations result in a complete lack of CFTR protein due to nonsense mutations or frameshift mutations, leading to severe cystic fibrosis phenotypes.
Explanation:
- Option B: Class II: Defective protein processing. Class II mutations, such as the common F508del mutation, produce CFTR protein that is misfolded and degraded before reaching the cell surface.
- Option C: Class III: Defective regulation. Class III mutations result in CFTR reaching the cell surface but being dysfunctional, as seen in mutations like G551D.
- Option D: Class IV: Defective conduction. Class IV mutations lead to a CFTR protein that is present and functional at the cell surface but has reduced chloride ion transport efficiency.
- Option E: Class V: Reduced protein quantity. Class V mutations result in decreased CFTR protein production but often result in a milder phenotype due to some functional protein being present.
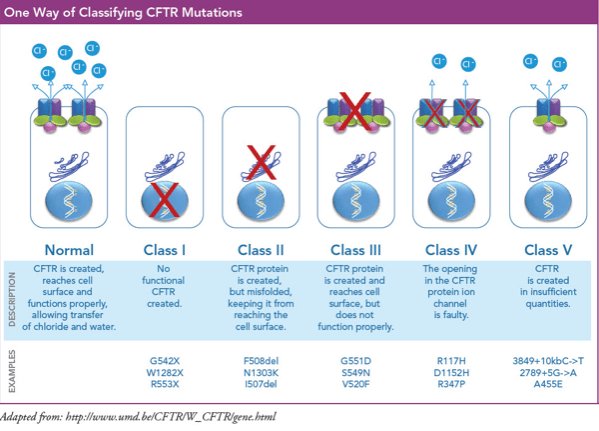
Question 89:
Correct answer: D
Pseudomonas aeruginosa is a common pathogen in VAP, particularly in patients with prolonged mechanical ventilation or prior antibiotic exposure. It is a gram-negative bacterium often associated with severe, healthcare-associated infections.
Explanation:
- Option A: Staphylococcus aureus (including MRSA) is a frequent cause of HAP, especially in ICU settings, but it is not as commonly associated with patients on prolonged ventilation compared to Pseudomonas aeruginosa.
- Option B: Streptococcus pneumoniae is a common cause of community-acquired pneumonia but is less likely in VAP, particularly after several days of mechanical ventilation.
- Option C: Haemophilus influenzae is another typical pathogen in community-acquired pneumonia and early-onset ventilator-associated pneumonia but less so in late-onset cases.
Option E: Legionella pneumophila causes atypical pneumonia and is associated with environmental water sources rather than mechanical ventilation.
